

Purpose
High jejunal atresia occurring near the ligament of Treitz is rare. It is a complicated type of small bowel atresia, and its treatment is challenging. Our study describes the clinical characteristics and proper management of high jejunal atresia.
Methods
We performed a retrospective review of seven neonates who underwent operations for high jejunal atresia between January 2000 and April 2021.
Results
The sex ratio showed a male predominance, and all patients were prenatally diagnosed with small bowel atresia. Six patients presented with a typical triple bubble appearance on the preoperative abdominal film. The location of the atresias were around the ligament of Treitz or less than 10 cm from the ligament of Treitz, and the types of atresia comprised three cases of type I, two of type IIIb, and two of type IV. Five of the seven patients underwent the operation without proximal enteroplasty. The median duration from operation to full feeding was 23 days, with three patients requiring more than a month to reach full feeding. There were no other operation-related complications. At the long-term follow-up, all patients tolerated oral feeding well.
Conclusion
This study indicates that high jejunal atresia close to the ligament of Treitz exhibits a high incidence of type I and complex types of atresia, and that primary anastomosis, without proximal enteroplasty, can be applied through surgical intervention.
High jejunal atresia occurring near the ligament of Treitz is rare. It is a complicated type of small bowel atresia, and its treatment is challenging. Our study describes the clinical characteristics and proper management of high jejunal atresia.
We performed a retrospective review of seven neonates who underwent operations for high jejunal atresia between January 2000 and April 2021.
The sex ratio showed a male predominance, and all patients were prenatally diagnosed with small bowel atresia. Six patients presented with a typical triple bubble appearance on the preoperative abdominal film. The location of the atresias were around the ligament of Treitz or less than 10 cm from the ligament of Treitz, and the types of atresia comprised three cases of type I, two of type IIIb, and two of type IV. Five of the seven patients underwent the operation without proximal enteroplasty. The median duration from operation to full feeding was 23 days, with three patients requiring more than a month to reach full feeding. There were no other operation-related complications. At the long-term follow-up, all patients tolerated oral feeding well.
This study indicates that high jejunal atresia close to the ligament of Treitz exhibits a high incidence of type I and complex types of atresia, and that primary anastomosis, without proximal enteroplasty, can be applied through surgical intervention.
Intestinal atresia is a well-known congenital anomaly, and its treatment outcome is usually excellent. However, some cases of small bowel atresia, such as multiple atresias, combined meconium peritonitis, or severe dilatation of the proximal atretic bowel, are not easy to treat [1, 2]. High jejunal atresia occurring near the ligament of Treitz is rare; it is a complicated type of small bowel atresia, and its treatment is challenging [3, 4, 5]. The dilated proximal jejunum is usually very short or even absent, so anastomosis with a small caliber distal jejunum can be extremely difficult.
Previous reports of high jejunal atresia have usually focused on surgical techniques for overcoming the diameter discrepancy of the proximal and distal bowels. Studies generally advocate the application of tapering enteroplasty to the dilated proximal bowel. However, various alternative techniques have been suggested for high jejunal atresia because the anatomical characteristics of the ligament of Treitz make it difficult to perform tapering enteroplasty [5, 6, 7, 8].
The clinical characteristics of high jejunal atresias are not yet well known, and a limited number of studies have reported on these [4, 8]. Their unusual location makes it hard to differentiate between an extremely high jejunal atresia, an atresia of the duodenojejunal junction, or a distal duodenal atresia [3, 9], and the surgical outcome might be different in each case.
The current study aims to provide information about the clinical characteristics of high jejunal atresia, its proper management, and outcomes.
The authors performed a retrospective review of the clinical data of 153 neonates who had undergone surgical treatment for small bowel atresia at our institution between January 2000 and April 2021. Of these patients, 48 had duodenal atresia and six had data inaccuracies, so these were excluded from the study. Of the remaining 99 jejunoileal atresias, we identified seven patients with high jejunal atresia with atretic lesions within approximately 10 cm of the ligament of Treitz. Their demographic characteristics, preoperative evaluations, operation findings, postoperative outcomes, and long-term prognoses were analyzed. The classification of the atresia was conducted according to the findings of a previous study [2].
The current study was approved by the Institutional Review Board of our hospital (4-2021-1364).
The patients’ characteristics are summarized in Table 1. The sex ratio indicates a male predominance; all patients were prenatally diagnosed with small bowel atresia. All patients were born without critical accompanying malformations, but five patients had associated diseases (Table 1). Only one patient weighed less than 2 kg at birth. Six patients showed a typical triple bubble appearance on the preoperative abdominal film, but this symptom was not observed in one patient (Fig. 1).
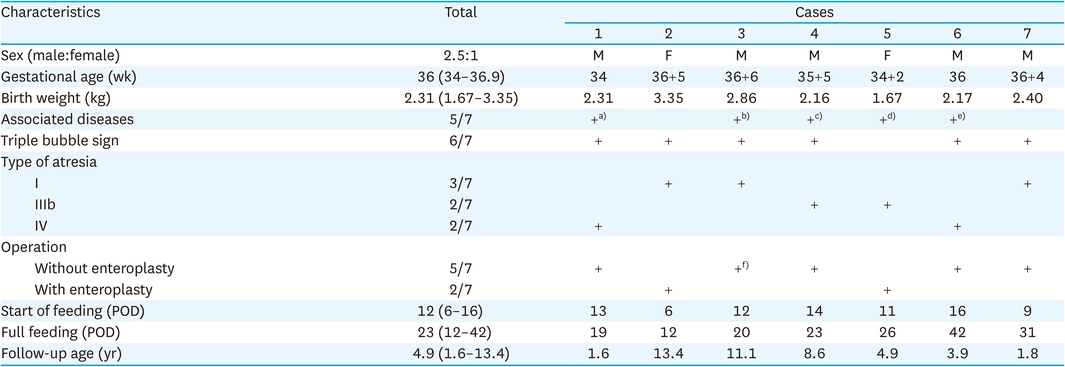
Table 1
Characteristics of patients
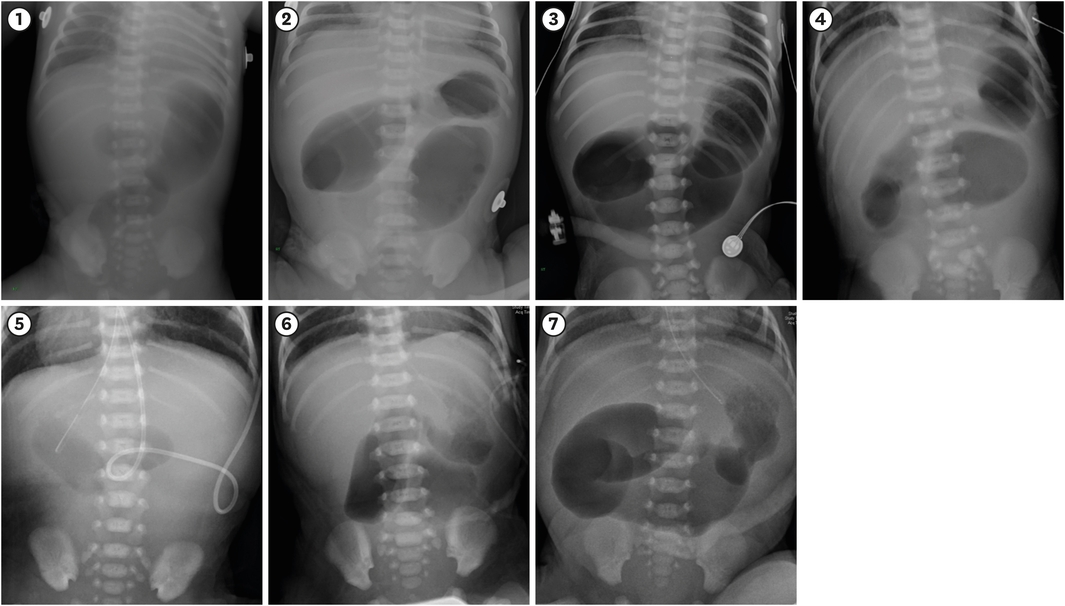
Fig. 1
Preoperative abdominal plain radiography. The number in the figure is the number of the individual case. A triple bubble appearance was observed in all cases except case 5.
All patients underwent one-stage corrective surgery between the first and fourth days after birth (median one day). The appearance of the atresia was classified as type I in three cases, IIIb in two cases, and IV in two cases. One patient (case 6) of type IV contained a feature of type I atresia (Fig. 2).
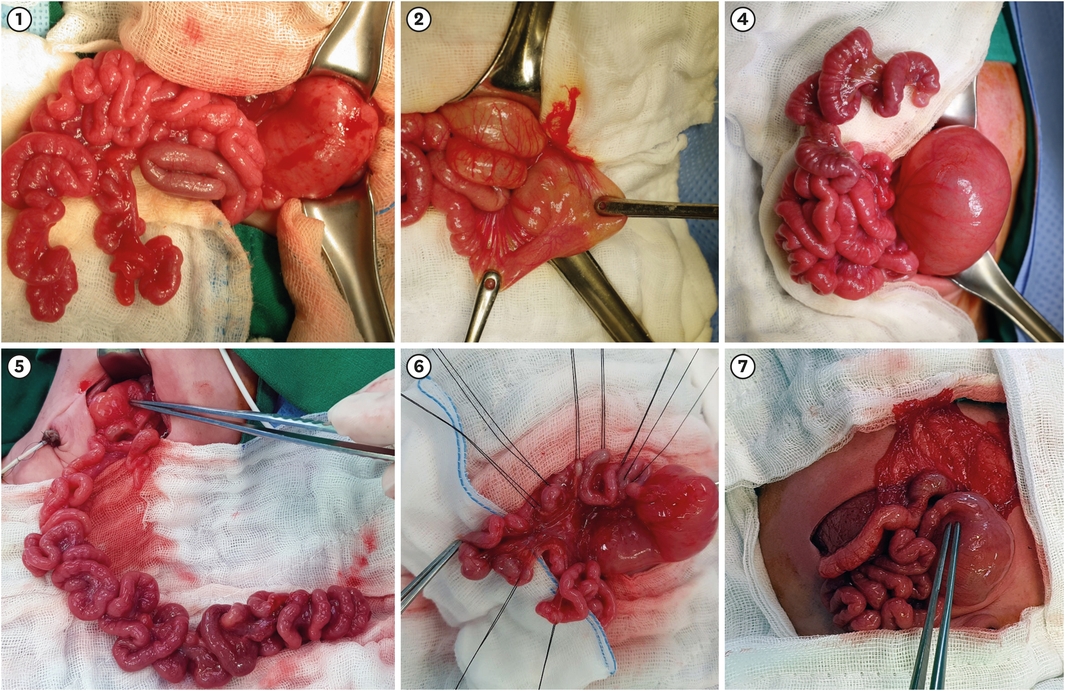
Fig. 2
Photographs of 6 high jejunal atresias. The number in the figure is the number of the individual case. Type I is observed in cases 2 and 7. Type IIIb is in cases 4 and 5. Type IV is in cases 1 and 6. Case 6 contained a feature of type I (No photograph available for case 3).
Five patients underwent anastomosis without proximal enteroplasty, but two patients required proximal enteroplasty. We did not have definite selection criteria for proximal enteroplasty; however, in case 1, we found a maximal contraction point in the proximal end of the atresia, which took on a nipple appearance during peristaltic movement. We decided to anastomose this lesion to the distal atretic bowel without proximal tapering enteroplasty, and the patient exhibited a good postoperative course. Following this case, we have considered the operation without proximal enteroplasty as one of the surgical treatment options.
The median duration from operation to full feeding was 23 days, and three patients required more than a month to reach full feeding. Apart from delays in full feeding, there were no other operation-related complications. All patients were followed up for more than one year, and they fed well without difficulty and had no additional admissions related to jejunal atresia.
Small bowel atresias include duodenal and jejunoileal atresia. Although its exact etiology is uncertain, jejunal atresia is known to be mainly caused by an intrauterine vascular accident, whereas duodenal atresia is known to be caused by a failure in recanalization [10, 11]. However, the classification of certain atresias as one of these two types is ambiguous. An atresia around the ligament of Treitz is often confusing and classified as a high jejunal atresia or an atresia on the distal end of the duodenum because the dilated end of the duodenum is pushed in the distal direction by the peristalsis and its gross appearance is similar to an extremely high jejunal atresia [6, 9, 12]. A jejunal atresia occurring near the ligament of Treitz might have the same characteristics as an atresia at the duodenojejunal junction, but they are likely to have different clinical characteristics from an atresia in the more distal part of the jejunum. Therefore, in this study, we defined high jejunal atresias as those occurring within approximately 10 cm of the ligament of Treitz [5] or at the duodenojejunal junction [9, 12].
The results of this study indicate that these atresias have specific characteristics. First, the study indicates a high incidence of type I atresias. The incidence of type I atresia is normally reported as between 6% and 23% of jejunoileal atresias [1, 2, 13, 14], but of the seven cases, we found four to be the feature of type I atresias (57.1%), including case 6. The other specific characteristic was the high incidence of complex atresias. This study included four such cases, two each of type IIIb and type IV atresias, which is higher than previous reports of their incidence among jejunoileal atresias [1, 2, 13, 14]. These two characteristics might be different from the characteristics of normal jejunoileal atresias.
However, our findings are not entirely different from those of previous studies, although these have been reported sporadically, and most were case reports. Yang et al. [8] reported that 51.2% (22/43) of high jejunal atresia was type I, and other case reports also indicated type I atresias in high jejunal atresia [7, 15, 16]. While these studies did not emphasize a high incidence of type I atresia, we believe this is a distinct characteristic of high jejunal atresia. Regarding the high incidence of complex atresias, Kazandjian et al. [4] reported that 6 of 13 high jejunal atresias were type IIIb atresias. The apple-peel appearance of the atresia was the prevalent finding in studies describing specific types of duodenal atresias [3, 9, 12, 17, 18]. However, these were not specifically mentioned as being high jejunal atresia but were described as duodenojejunal atresia or just duodenal atresia. These reports and the results of the present study suggest that the pathophysiology of high jejunal atresia differs from that of typical small bowel atresia.
In diagnosing high jejunal atresia, the triple bubble sign was a reliable finding in this study [15, 16, 19]. The “triple bubble” reflects the air shadows of the stomach, the duodenal bulb, and the proximal jejunum, and it is an excellent indicator of high jejunal atresia. In this study, six of the seven cases had a definite triple bubble appearance on a plain X-ray, although one case lacked this clearly defined triple bubble. In this case, the X-ray may have been taken before full inflation of the proximal atretic bowel. The triple bubble sign is a simple and helpful diagnostic tool for awareness of high jejunal atresia.
The surgical treatment of high jejunal atresia is more challenging than that of small bowel atresia. The proximal bowels of the atresia are usually very dilated, and they need to be resected due to abnormal motility and functional obstruction after anastomosis. Tapering enteroplasty or bowel plication are other options for managing bowel dilatations when the resection is extensive and could result in short bowel syndrome. These techniques are also applicable in high jejunal atresias with minimal proximal bowel length [8, 20]. However, enteroplasty in the area of the ligament of Treitz is not easy due to its anatomical characteristics, and some anatomical deformation is necessary to achieve enteroplasty [5, 6]. In this study, we performed end-to-end anastomosis in five of the seven cases. In case 1, we tried primary anastomosis because of difficulties in applying proximal enteroplasty and an observation of the maximal contraction point of the proximal end of the atresia. After our experience with this case, we tried primary anastomosis without enteroplasty in the other cases, and the results were not disappointing. Therefore, we suggest that primary anastomosis is appropriate if it is possible to anastomose in the maximal contraction area. However, patients should be selected carefully for this surgical method, and if enteroplasty is reasonably possible, it is preferable to perform it.
This study has some limitations. As this was a retrospective study, the selection of surgical methods was inconsistent, and the pediatric surgeons conducted the postoperative treatments on an individual basis. Statistical analysis was not possible due to the small number of patients. However, despite these limitations, this is a very rare study in that it analyzes high jejunal atresia, and we believe that the results of this study will help in the treatment of high jejunal atresia.
In summary, type I and complex types of atresia are common in high jejunal atresias, and primary anastomosis without proximal enteroplasty could be applied as a surgical treatment. The results of the study suggest that high jejunal atresia close to the ligament of Treitz has different clinical characteristics than those of common jejunal atresia.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: J.H.J., H.I.G., O.J.T.
Data curation: J.H.J., H.I.G., O.J.T.
Methodology: J.H.J.
Supervision: O.J.T.
Validation: H.I.G., O.J.T.
Writing - original draft: J.H.J.
Writing - review & editing: O.J.T.
