

Purpose
Kidney transplantation (KT) in small children is known to be associated with increased risk of surgical complications that may potentially lead to graft loss. KT in children weighing 15 kg or less are considered to be most technically challenging. We present our transplant center's experience with KT in this cohort of children.
Methods
We retrospectively reviewed our transplant center's KT database from January 1994 to July 2019. Recipients’ and donors' data were collected for analysis.
Results
From January 1995 to July 2019, 69 cases of KT were performed in recipients ≤18 years. We identified 9 children (11.8%) who weighed ≤15 kg at the time of KT. There were 4 boys and 5 girls. Median age of recipients was 4.0 years (range 16 months–7 years). Median weight at KT was 14.0 kg (range, 11–15 kg). 3 cases were living-donor KT and 6 cases were deceased-donor KT. Median weight of the kidney allograft was 106 g (range, 65–235 g). The allograft was implanted intraperitoneally in 6 cases and extraperitoneally in 3 cases. Postoperative vascular complication occurred in 1 patient (arterial anastomosis stenosis). Graft loss occurred in 2 patients, due to renal artery stenosis and chronic allograft nephropathy. Graft survival was 88.9% and 88.9% at 1 and 5 years, respectively. Mean followup was 91.6 months. Graft survival of children who weighed ≤15 kg at the time of KT was not different compared to children who weighed more than 15 kg.
Conclusion
KT in small children weighing ≤15 kg is technically challenging. However, with comprehensive care by a pediatric transplant specialist, these challenges may be overcome and lead to good transplant outcomes.
Kidney transplantation (KT) in small children is known to be associated with increased risk of surgical complications that may potentially lead to graft loss. KT in children weighing 15 kg or less are considered to be most technically challenging. We present our transplant center's experience with KT in this cohort of children.
We retrospectively reviewed our transplant center's KT database from January 1994 to July 2019. Recipients’ and donors' data were collected for analysis.
From January 1995 to July 2019, 69 cases of KT were performed in recipients ≤18 years. We identified 9 children (11.8%) who weighed ≤15 kg at the time of KT. There were 4 boys and 5 girls. Median age of recipients was 4.0 years (range 16 months–7 years). Median weight at KT was 14.0 kg (range, 11–15 kg). 3 cases were living-donor KT and 6 cases were deceased-donor KT. Median weight of the kidney allograft was 106 g (range, 65–235 g). The allograft was implanted intraperitoneally in 6 cases and extraperitoneally in 3 cases. Postoperative vascular complication occurred in 1 patient (arterial anastomosis stenosis). Graft loss occurred in 2 patients, due to renal artery stenosis and chronic allograft nephropathy. Graft survival was 88.9% and 88.9% at 1 and 5 years, respectively. Mean follow-up was 91.6 months. Graft survival of children who weighed ≤15 kg at the time of KT was not different compared to children who weighed more than 15 kg.
KT in small children weighing ≤15 kg is technically challenging. However, with comprehensive care by a pediatric transplant specialist, these challenges may be overcome and lead to good transplant outcomes.
Kidney transplantation (KT) is the treatment of choice in children with chronic kidney disease (CKD) stage 5 and improves survival, growth and quality of life in children than dialysis [1]. Mortality of pediatric patients on dialysis increases with younger age, with 13.6 deaths per 100 patients aged <1 year [2]. Thus, younger children would benefit most when KT is performed with technical precision and an adequate kidney graft. KT in small children weighing 15 kg or less is generally perceived to be technically challenging with an increased risk of surgical complication, which may potentially lead to severe morbidity, graft loss or decreased overall survival [3, 4, 5]. Potential surgical complications are believed to be the result of smaller vasculature, imbalance between adult donor organ and pediatric recipient body, and congenital anomalies in the recipient. However, outcomes of KT in low-weight pediatric recipients compared to larger children are scarcely reported in the literature. Our study aimed to analyze the result of KT in children weighing 15 kg or less in a single center in Korea, focusing on graft failure and overall survival in this cohort of pediatric KT recipients.
We retrospectively reviewed the medical records of 69 recipients 18 years of age or younger at the time of KT performed at Samsung Medical Center (Seoul, Korea) from January 1994 to July 2019. According to the weight of the patient at the time KT was performed, the analysis was divided into 2 groups: recipients exceeding 15 kg and recipients weighing 15 kg or less. Donor characteristics, cause of CKD, surgical complications, graft survival and patient survival data were collected. Graft loss was defined as initiation of renal replacement therapy following KT or death of the recipient with a functioning graft.
The kidney was placed extraperitoneally when sufficient space was available in the iliac fossa. Extraperitoneal approach was achieved through a J-shaped pararectal incision and the iliac vessels were exposed to allow for vascular anastomosis. Intraperitoneal approach was achieved through a midline incision. In either intraperitoneal or extraperitoneal position, the right side was preferred. Site of vascular anastomosis was selected based on the position of the graft vessels relative to the recipient’s vasculature. Anastomoses were done in end-to side fashion, unless the internal iliac artery was used. Ureteral implantation was done using the Lich-Gregoire technique and no ureteral stents were used.
Interleukin-2 receptor antagonist (basiliximab) was used as induction immunosuppression before restoring blood flow to the graft. As for maintenance therapy, tacrolimus (or cyclosporin), mycophenolate mofetil and steroids were the primary agents for immunosuppression. Methylprednisolone 20 mg/kg was administered intravenously before restoring blood flow to the allograft. Steroids were tapered over 7 days postoperatively and oral prednisolone was maintained for 1 month. Calcineurin inhibitors were started immediately after the operation and subsequently adjusted to maintain trough concentrations at 10–12 ng/mL for tacrolimus and 100–150 ng/mL for cyclosporin. Mycophenolate mofetil was continued from postoperative day 1.
Categorical variables were verified by χ2 test or Fisher's exact test. Continuous variables were analyzed by performing the Mann-Whitney U test. Kaplan-Meier analysis and log-rank test were used to compare variables regarding graft survival. Statistical significance was set at p<0.05. Statistical analysis was performed using SPSS software version 20 (SPSS Inc., Chicago, IL, USA).
At the time of KT, 9 patients (13%) weighed ≤15 kg, and 60 patients weighed more than 15 kg. Of the 9 patients weighing ≤15 kg, 4 (44.4%) were male and 5 were female. 6 cases were deceased donor KT and 3 cases were living donor KT. The age at KT was 4.44±2.12 years in the weight ≤15 kg group, which was significantly younger than 13.8±4.12 years in the weight >15 kg group. The causes of KT showed no difference between the 2 groups. Graft failure was 22.2% in the weight ≤15 kg group and 26.7% in the weight >15 kg group, and there was no statistical difference between the 2 groups (Table 1). Median follow-up was 91.6 months (range, 5–271 months).
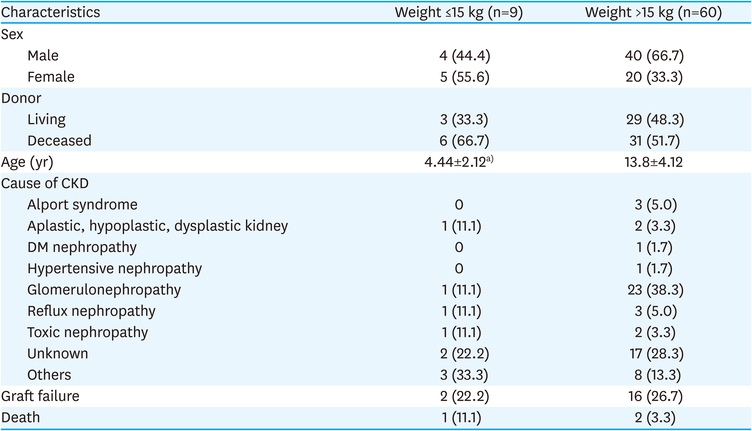
Table 1
Characteristics of pediatric kidney transplant recipients
Median weight of the kidney allograft was 106 g (range, 65–235 g). The allograft was implanted intraperitoneally in 6 cases and extraperitoneally in 3 cases. Arterial anastomosis was performed to the internal iliac artery in 1 case, the aorta in 5 cases, and to the external iliac artery in 3 cases. Vein anastomosis was performed to the inferior vena cava in 6 cases and the external iliac vein in 3 cases (Table 2).
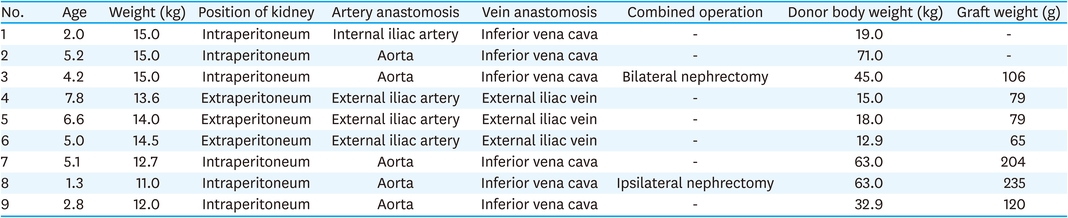
Table 2
Operative characteristics of weight ≤15 kg recipients
Postoperative surgical complications occurred in 1 patient (arterial anastomosis stenosis, which lead to graft loss and eventual recipient mortality) in the weight ≤15 kg group and in 2 patients (bleeding and urine leak) in the weight >15 kg group. Graft loss occurred in 2 patients, due to renal artery anastomosis stenosis and chronic allograft nephropathy in the weight ≤ 15 kg group (Table 3).

Table 3
Cause of graft failure
Graft survival was 88.9% and 88.9% at 1 year and 5 years, respectively (Fig. 1A). Graft survival of children who weighed ≤15 kg at the time of KT was not different compared to children who weighed more than 15 kg (p=0.832). Patient survival was also not significantly different between the 2 groups (p=0.234, Fig. 1B).
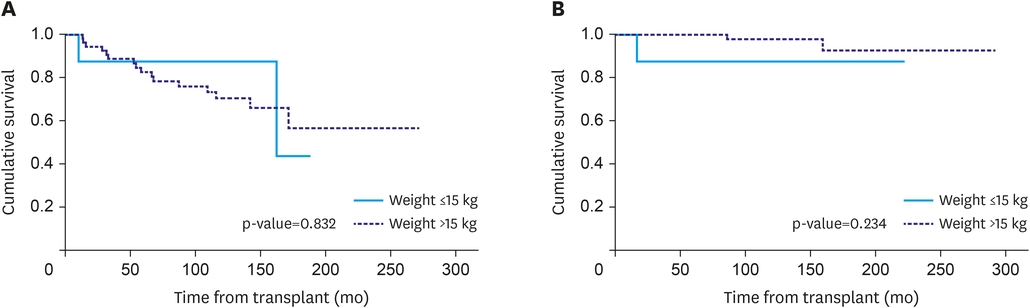
Fig. 1
(A) Graft survival according to recipient weight. (B) Overall survival according to recipient weight.
KT in small children is technically demanding for the pediatric transplant surgeon and the risks and benefits of KT in low-weight recipients are still controversial [3, 5, 6, 7, 8, 9, 10]. An absolute lower limit of body weight does not exist for KT to be safely performed, nor is there a clear consensus as to the definition of “low-weight” pediatric recipients of KT. However, previous publications outline children weighing less than 15 kg as low-weight and most authors consider the lower limit for pediatric KT to be 10 kg [5, 6, 7]. It is noteworthy that the mortality for pediatric patients on dialysis is the highest in smaller children and the survival benefits of children receiving KT compared to remaining on dialysis are well documented [1]. In a study by Gillen et al., [1] the relative risks of mortality in pediatric KT recipients were lower than those of children staying on the transplant waitlist in all 3 age groups (age, 0–5; age, 6–12; age, 13–18) up to 36 months post-transplant, apart from a brief period of increase in risk during the first 6 months in recipients aged 0–5. Thus, the risks and benefits of performing KT should be carefully considered in each patient with regard to their age, body weight, and underlying comorbidities.
A general perception when considering KT in low-weight recipients is that it is associated with increased risk of vascular complications and subsequent inferior graft outcome. Although the low-weight recipient with smaller vessels and decreased arterial inflow may seem to predispose to vascular thrombosis, there is no concrete evidence to support this predilection. Published literature on the outcome of pediatric KT recipients weighing 15 kg or less report the incidence of vascular complications to be between 2% and 10% [2, 3, 5, 6, 8, 9]. Our experience was one case of arterial anastomosis site stenosis (11.1%) leading to graft failure among 9 recipients weighing 15 kg or less, and comparable graft survival and overall survival compared to pediatric recipients weighing more than 15 kg. The reported incidence of vascular complications in pediatric KT recipients overall was 4%–18% [11, 12] and most studies failed to show significant correlation between recipient age or weight and increased risk of vascular complications following KT. However, younger age of the donor, specifically donor age younger than 6 years was shown to be associated with increased risk of vascular complications following pediatric KT [13, 14].
Extraperitoneal placement in the iliac fossa is the preferred position of a kidney allograft in adult and pediatric KT recipients alike. Advantages of the extraperitoneal approach include minimal gastrointestinal complications, preservation of the peritoneal cavity, and fixation of the kidney allograft with minimal potential for twisting of the allograft around its vascular axis [15, 16]. However, in small children the iliac fossa may not have sufficient capacity for a larger kidney allograft from an adult donor and a transperitoneal approach must be elected [17, 18]. The lower limit of age or weight of the recipient does not exist in which extraperitoneal approach would not be sufficient and transperitoneal approach must be considered. With growing experience with application of the extraperitoneal approach in smaller children, more transplant centers are readily utilizing this approach in children weighing less than 15 kg [3, 4, 15, 16]. It is believed that the weight limit in extraperitoneal approach is closely related to the size discrepancy between recipient and donor or recipient and kidney allograft [5]. Our experience was consistent with this concept, as all 3 of the recipients in which extraperitoneal approaches were taken involved small donors (weight <20 kg) and small grafts (weight <100 g).
We believe the findings in this study are valid but there are apparent limitations. It is a retrospective analysis which is prone to biases in collection and interpretation of the data. Secondly, it is a single-center study involving a limited number of patients from our transplant center. This limitation may lead to bias that may not be applicable to other centers with differing circumstances and experiences.
In conclusion, KT in small children weighing 15 kg or less is technically challenging. However, with comprehensive care by a pediatric transplant specialist, these challenges may be overcome and lead to transplant outcomes comparable to those of larger children.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: L.S., O.C.
Data curation: L.S., L.K.W., P.J.B.
Formal analysis: L.O.
Supervision: L.S., P.J.B.
Writing - original draft: L.C.H., L.S., O.C, L.O.
Writing - review & editing: L.S., O.C.
