

Purpose
Patients with esophageal atresia (EA) often have feeding problems due to esophageal dysmotility, gastroesophageal reflux, and dysphagia, which can delay growth in children. The purpose of this study was to investigate whether proper growth is achieved during the early childhood of patients with EA and to predict associated factors.
Methods
Clinical data of patients with EA who underwent corrective surgery between 2014 and 2017 were collected retrospectively. We analyzed a total of 17 patients who were followed up for at least two years after surgery, except for patients with long-gap and type E EA. The median follow-up period was 979.0 months. We analyzed the weight, height, and weight-forheight (WFH) as z-scores. Linear regression analysis was performed to determine the factors affecting WFH at two years of age.
Results
Of the 17 patients, 11 underwent open surgery and six underwent thoracoscopic surgery. The median time to full feeding was approximately 14 (range, 12.0–53.0) days. In patients with anastomotic stenosis, esophageal balloon dilatation was performed 1–6 times. There was no mortality in our study, and the median follow-up period was 979 days. The mean height was 49.0 cm, the mean weight at birth was 2.69 kg, and the z-scores were −0.55 and −1.44, respectively. The WFH z-score decreased from −1.66 at birth to −1.82 one week postoperatively; however, it improved to −0.2 after six months. In multivariate linear regression analysis, only WFH at birth was a significant variable for WFH at two years of age.
Conclusion
Patients with EA tend to have lower weight and WFH at birth, which worsened after surgery; however, six months after surgery, both weight and WFH recovered to the 50th percentile. The factors that influence WFH at two years of age were significantly related to WFH at birth.
Patients with esophageal atresia (EA) often have feeding problems due to esophageal dysmotility, gastroesophageal reflux, and dysphagia, which can delay growth in children. The purpose of this study was to investigate whether proper growth is achieved during the early childhood of patients with EA and to predict associated factors.
Clinical data of patients with EA who underwent corrective surgery between 2014 and 2017 were collected retrospectively. We analyzed a total of 17 patients who were followed up for at least two years after surgery, except for patients with long-gap and type E EA. The median follow-up period was 979.0 months. We analyzed the weight, height, and weight-for-height (WFH) as z-scores. Linear regression analysis was performed to determine the factors affecting WFH at two years of age.
Of the 17 patients, 11 underwent open surgery and six underwent thoracoscopic surgery. The median time to full feeding was approximately 14 (range, 12.0–53.0) days. In patients with anastomotic stenosis, esophageal balloon dilatation was performed 1–6 times. There was no mortality in our study, and the median follow-up period was 979 days. The mean height was 49.0 cm, the mean weight at birth was 2.69 kg, and the z-scores were −0.55 and −1.44, respectively. The WFH z-score decreased from −1.66 at birth to −1.82 one week postoperatively; however, it improved to −0.2 after six months. In multivariate linear regression analysis, only WFH at birth was a significant variable for WFH at two years of age.
Patients with EA tend to have lower weight and WFH at birth, which worsened after surgery; however, six months after surgery, both weight and WFH recovered to the 50th percentile. The factors that influence WFH at two years of age were significantly related to WFH at birth.
Malnutrition is a major issue in chronically ill children [1]. Infants and children under 3 years of age have higher risk of malnutrition due to neurological development and growth spurt [2]. Children, who needed a long period of hospitalization, suffered from malnutrition [3]. Children with congenital cardiac anomalies tend to have a higher rate of malnutrition due to longer hospitalization and repeated surgery, which is associated with increased morbidity and mortality rates, including frequent hospitalization and poor surgical outcomes [4]. Malnutrition has been suggested to result in impaired growth status, poor school performance, and reduced intellectual achievement.
Among the congenital anomalies, gastrointestinal anomalies, such as esophageal atresia (EA), duodenal atresia, and imperforate anus, can affect the feeding capacity due to impaired gastrointestinal tract. Therefore, gastrointestinal anomalies pose a significant risk for malnutrition. EA with or without tracheoesophageal fistula (TEF) is one of the most common congenital anomalies in pediatrics and is characterized by a complete discontinuity of the esophagus. The prevalence of EA was reported to be 1 in 4,099 births [5]. While malnutrition has been associated with EA, there have been no reports on the growth outcome of EA in Korea. In this study, we aimed to investigate whether proper growth is achieved during the early childhood of patients with EA. In addition, the factors associated with growth outcomes were investigated.
We retrospectively collected data of patients with EA who had undergone corrective surgery at Seoul National University Hospital from January 2014 to December 2017. In this study, 20 patients with type C EA who had EA with distal TEF were included. We did not include type A EA because treatment plan was different between type A and C EA. We collected data on patient characteristics, combined anomalies, and operation and growth outcomes. We analyzed 17 patients who were followed up for at least two years after their operation. In our hospital, we followed up with patients with EA at the outpatient clinic with growth assessments and questionnaires regarding eating habits and symptoms during every visit. Weight and height were measured using methods previously reported by the World Health Organization (WHO) [6]. The z-scores for weight, height and weight-for-height (WFH) were calculated using the WHO Anthro Survey Analyser.
To assess the severity of pediatric malnutrition, we compared the height, weight, and WFH ratio using z-scores. Mild malnutrition was defined as a z-score between −1 and −1.9; moderate malnutrition was defined as a z-score between −2 and −2.9; and severe malnutrition was defined as a z-score ≤3 z-score [7]. The time of operation, time until oral feeding post-operation, time until full feeding, length of hospital stays, anastomosis leakage, anastomosis stenosis, re-operations, and mortality rates were used to determine outcomes. Before 2016, 11 patients had undergone open EA/TEF repair. Since 2016, we have performed thoracoscopic repairs in all six patients with type C EA. There was no difference in operative procedure between thoracotomy and thoracoscopic repair.
To analyze the growth outcomes of patients with EA, we measured their weight and height at birth, on the day of operation, at one week, six months, one year, and two years after surgery. We compared the height, weight, and WFH ratio using z-scores. In addition, to identify the factors associated with postoperative two-year growth outcomes, we performed linear regression analysis using variables such as WFH at birth, time until full feeding, and postoperative complications (stenosis, leakage, and gastroesophageal reflux [GER]) at seven days, one year, and two years postoperatively.
R version 3.4.4 was used for statistical analysis. All continuous variables are presented as the median values with the interquartile range. A normality test was first performed to test the significance of continuous variables. Univariate linear regression analysis was performed. We then used the significant variables under 0.2 for the multivariate analysis. The p-values <0.05 were considered statistically significant.
Of the 17 patients, nine were male (52.9%) and eight were female (47.1%). The average gestational age was 37.3±3.1 weeks (Table 1). At birth, the mean height and weight were 48.4±4.0 cm and 2.7±0.6 kg, respectively. In terms of z-scores, the average birth heights and weights were −0.55±2.2 and −1.44±1.6, respectively. The z-score of WFH was −1.67±2.1 at birth. Seven patients were diagnosed with VACTERL syndrome (vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities). All patients also had cardiac anomalies.
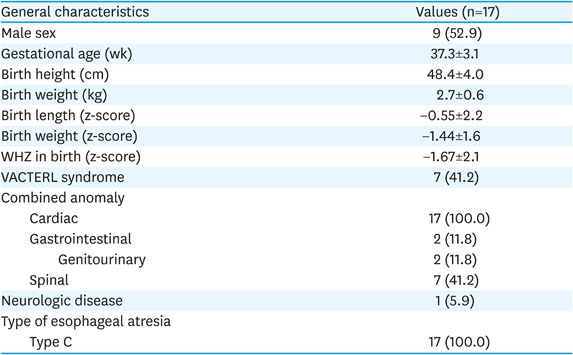
Table 1
General characteristics
On average, the patients underwent surgery 2.3 days after birth. The mean operation duration was 115.0 (69.0–245.0) minutes (Table 2). We routinely performed a postoperative contrast study seven days after the operation. If there was no contrast leakage at the anastomosis site, the patients were started on a diet. The average time until full feeding was 14 days. There were no cases of mortality in this study. However, three patients required re-operation, two of whom were diagnosed with a recurrent fistula, and one patient was diagnosed with a tracheobronchial remnant.
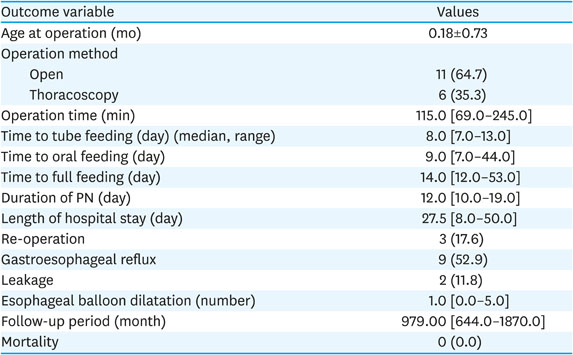
Table 2
Surgical results after primary repair of type C EA
Following a consistent schedule, we monitored the patients' body weight and height (Table 3). One week after the operation, the mean body weight z-score decreased to −1.79±1.75 compared to −1.67±1.82 on the day of the operation. For the WFH ratio, we observed a similar trend, which showed that the height z-score decreased from −1.66±2.09 to −1.82±1.15. Subsequently, we measured anthropometry at six months, one year, and two years old in the outpatient clinic. At the age of six months, all indicators for growth improved. After two years, the average weight z-score recovered to −0.41±1.31, indicating that the growth of children with EA almost reached the 50th percentile in weight. The WFH z-score also recovered up to −0.08±0.98 at the two-year follow-up.

Table 3
Growth outcomes after esophageal atresia repair
We investigated variables affecting the WFH z-score at two years of age, including WFH at birth, time until full feeding, stenosis/leakage at seven days after operation, and stenosis/gastroesophageal reflux at one year after surgery (Table 4). After univariate linear regression analysis, WFH at birth, time until full feeding, and stenosis one year after operation were significant factors associated with growth at two years of age. However, when we performed multivariate analysis, the WFH z-score at birth was the only significant factor for low WFH at two years of age in children with EA.
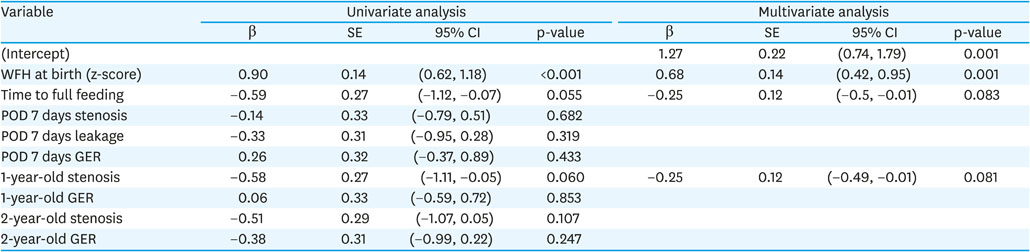
Table 4
The effect of variables on WFH in z-score at 2 years old (result of linear regression analysis)
In a previous retrospective study, a 95% survival rate of EA was reported [8]. Many researchers wondered about the patient's quality of life after surgery, including neurologic, pulmonary, and growth outcomes and any feeding problems [9, 10, 11]. Considering the report by Gottrand et al. [12], the most important cause of nutritional problems in patients with EA was dysphagia. Dysphagia developed in these patients due to esophagitis, GER, esophageal dysmotility, anastomosis stricture, aspiration tendency, and oral avulsion. The rate of GER after EA repair was reported to be between 20% and 63%. Friedmacher et al. [13] reported a 79.3% incidence of GER after EA/TEF repair, which was higher than that in a previous study, and our study showed 52.9% of GER in a contrast study. Dysphagia is considered a complication in 22%–50% of patients [14].
Although dysphagia is an important factor in nutritional outcomes, there are other factors that determine feeding difficulty. Overall feeding difficulty in EA children was reported in between 6% and 52% [15]. The predictors for feeding difficulty in patients with EA were reported in previous studies as long-gap EA, CHARGE association [16], and neurological abnormalities [17, 18]. If either dysphagia or feeding problems, which decreased their energy intake, were present for a prolonged period in patients with EA, they could suffer from malnutrition and growth failure. However, there are few reports about the association between EA and growth failure. Lacher et al. [19] performed a retrospective observational study in a single institute, which involved patients who had been diagnosed with EA over the last 22 years. They observed the body weight of patients until the age of six years. A total of 67% of the patients had a body weight lower than the 25th percentile of the general population. However, the group in this study was heterogeneous, in that they were included regardless of the type of EA. Even though the authors reported that patients with long-gap EA had lower weights than the other groups, there was no definite growth outcome in patients with type C EA. On the other hand, another study found that 16% of patients who were overweight [20]. Therefore, data on the growth outcome of patients with EA after primary repair are not conclusive. In the present study, we excluded patients with long-gap EA, who had a high probability of combined chromosomal anomalies and associated growth retardation, and only analyzed patients with type C EA. We found that they grew up as much as −0.19 z-score in height and −0.53 z-score in weight at the last follow-up around the age of two years. Regarding the current definition of malnutrition by the World Health Organization, these patients had a risk of undernutrition, but not definite malnutrition status. Our results showed better outcomes than previous studies.
In many previous studies, almost all growth outcomes were analyzed using only body weight. Height is an important parameter of chronic malnutrition [21]. Chronic malnutrition is defined as a −2 z-score in length for age [22]. We used patient height data to calculate the height-for-age and WFH to confirm whether the patient had acute or chronic malnutrition.
To the best of our knowledge, the factors that affect growth outcomes in patients with type C EA remains to be elucidated. However, some studies have investigated the factors associated with dysphagia. Even though dysphagia is one of the main causes of undernutrition and growth failure, there are still other factors. Patients with EA suffer from GER, stenosis, and functional problems such as dysmotility of the esophagus [14]. In our institute, we prescribed proton pump inhibitors for patients with GER; however, no patient underwent fundoplication. For patients with dysphagia due to anastomosis stenosis, we performed esophageal balloon dilatation. We evaluated GER and stenosis at one and two years of age and analyzed them as predictors of growth. Children with GER could suffer from failure to thrive [23]. However, even though patients suffered from GER and stenosis, they were not associated with growth outcomes in this study. A limitation of this study was that we followed up patients for only two years and did not evaluate a dysphagia symptoms.
Long-term growth outcomes after EA/TEF repair should be investigated in future studies. Our observations indicate that growth outcomes worsened immediately after EA/TEF repair but recovered by two years of age. WFH at birth is the only predictor of growth outcomes in patients with type C EA.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.D.,K.H.Y.
Data curation: L.C.
Formal analysis: K.D.
Investigation: Y.J.K.
Methodology: Y.H.B.
Supervision: K.H.Y.
Visualization: K.D.
Writing - original draft: K.D., L.C.
Writing - review & editing: K.D., K.H.Y.
