

Purpose
The aim of our study was to provide informative data for surgically treated preterm infants with incarcerated inguinal hernia (IH) in the neonatal intensive care unit (NICU).
Methods
Medical records of 9 preterm infants in NICU who underwent IH repair before NICU discharge between January 2011 and June 2020 were reviewed. The definition of incarcerated IH used was irreducible IH even by pediatric surgeon regardless of the use of sedation. The incarceration rate was calculated and informative data for incarcerated IH patients were collected.
Results
Of 237 IH patients, 9 were diagnosed with an incarcerated IH and underwent emergency repair. At diagnosis of IH, the median age, the median postmenstrual age, and the median body weight were 22 days, 29.7 weeks, and 1,090 g, respectively. The diagnosis interval from IH to incarceration was ranged from 6 to 51 days, and none of them died of surgical procedure-related complications. Strangulation occurred in 4 patients and was treated with small bowel resection and enterostomy.
Conclusion
This study provided informative data for incarcerated IH in preterm infants successfully treated surgically. Close observation is more necessary because the incarceration rate during observation of preterm infants with IH in the NICU is as high as 3.8%.
The aim of our study was to provide informative data for surgically treated preterm infants with incarcerated inguinal hernia (IH) in the neonatal intensive care unit (NICU).
Medical records of 9 preterm infants in NICU who underwent IH repair before NICU discharge between January 2011 and June 2020 were reviewed. The definition of incarcerated IH used was irreducible IH even by pediatric surgeon regardless of the use of sedation. The incarceration rate was calculated and informative data for incarcerated IH patients were collected.
Of 237 IH patients, 9 were diagnosed with an incarcerated IH and underwent emergency repair. At diagnosis of IH, the median age, the median postmenstrual age, and the median body weight were 22 days, 29.7 weeks, and 1,090 g, respectively. The diagnosis interval from IH to incarceration was ranged from 6 to 51 days, and none of them died of surgical procedure-related complications. Strangulation occurred in 4 patients and was treated with small bowel resection and enterostomy.
This study provided informative data for incarcerated IH in preterm infants successfully treated surgically. Close observation is more necessary because the incarceration rate during observation of preterm infants with IH in the NICU is as high as 3.8%.
Inguinal hernia (IH) is a common condition in premature and low birth weight infants, usually due to patent processus vaginalis, which normally closes in the last week of gestation [1, 2, 3]. They have multiple risk factors for IH, including raised intra-abdominal pressure from mechanical ventilation and bronchio-pulmonary dysplasia, and decreased abdominal muscle tone related to prematurity and poor nutrition. The incidence of IH increases with lower gestational age and birth weight; 3–5% in term infants up to 13% in infants less than 33 weeks gestation, and 14–30% in very low birth weight (less than 1,500g) [1].
The optimal timing of IH repair in premature infants is not clear. Technical challenges, co-morbid conditions, and potential anesthetic and surgical complications in these extremely small neonates motivate delaying of the operation [4, 5]. Proponents of early surgery advocate early repair to avoid the risk of strangulation and testicular atrophy during the waiting period [6], while others support late repair as an infant's tolerance to general anesthesia improves with maturation [7]. There are concerns about the increase in the incarceration rate as the operation is delayed, but there are few papers showing a statistical difference in this.
We provided informative data for preterm infants who underwent emergency repair for incarcerated IH in the neonatal intensive care unit (NICU).
Medical records of preterm infants (defined as born alive before 37 weeks of gestation) in NICU who underwent IH repair between January 2011 and June 2020 were retrospectively reviewed. In our center, we prefer to perform IH repair shortly before the infant's anticipated discharge from the NICU. In total, 237 patients underwent IH repair during their NICU hospitalization. Among these patients, 9 cases of incarcerated IH repair were performed, and all 9 cases were emergency surgery. All 9 cases described in the paper were performed as open surgery. Incarcerated IH was defined as irreducible IH even by pediatric surgeons regardless of the use of sedation.
Patient demographics, such as gestational age, birth weight, sex, Apgar scores at 1 and 5 minutes, IH side, were collected. Data about the postnatal age, postmenstrual age (PMA), and body weight at diagnosis of IH and IH repair were collected. We also investigated herniated contents, strangulation, combined surgery at IH repair.
All statistical analyses were performed using SPSS software (version 27.0 for Windows; SPSS Inc., Chicago, IL). Results were presented as median with range. This study was approved by the Institutional Review Board (IRB) at Samsung Medical Center (IRB No. 2021-09-124).
Of 237 preterm IH patients, 9 were diagnosed with an incarcerated hernia and underwent emergency IH repair. The mean gestational age at birth was 26.7 weeks, and the median birth weight was 920 g. The median value of age, PMA, and body weight at surgery were 34 days, 31.0 weeks, and 1,430 g, respectively. Preoperatively, 6 (67%) patients had bronchopulmonary dysplasia (BPD) and all required mechanical ventilation. Of these 6 patients, 2 patients combined intraventricular hemorrhage (IVH) over grades III–IV, blood culture-proven sepsis, and necrotizing enterocolitis; 1 patient had ductus arteriosus requiring surgical ligation with the cardiac anomaly in addition to IVH; 1 patient was diagnosed with blood culture-proven sepsis; and the other 2 patients had BPD alone. The median postoperative follow-up period was 26.8 months. During follow-up, recurrence of IH and postoperative complications such as hematoma and wound infection were not observed in incarcerated IH patients (Table 1).
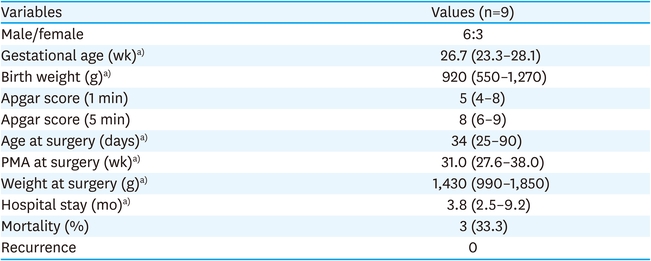
Table 1
Patient demographics
The detailed characteristics and treatment outcomes of the 9 patients are shown in Table 2. The median value of age, PMA, and body weight at diagnosis of IH were 22 days, 29.7 weeks, and 1,090 g, respectively. After the diagnosis of IH, incarceration occurred median of 9 days later. The emergency surgery was performed on the same day of the occurrence of incarceration. There were 7 patients with unilateral IH. All 3 female infants had genital organ herniation, such as ovary, ovarian cyst, and uterus. Strangulation occurred in 4 patients with small bowel or colon herniation. Small bowel resection, enterostomy were performed in strangulation cases. Among 9 patients, 3 (33.3%) died after 1.3, 2.2, and 5.8 months respectively. None of the deaths were related to the procedure for IH repair. Three mortality cases were caused by complex neonatal comorbidity and multi-organ failure, consequently. The first infant suffered from pulmonary complications such as recurrent pneumothorax and pneumonia with prolonged ventilator use due to severe BPD and died 5.8 months after surgery. The second infant died 1.3 months after surgery because of deterioration of renal function combining persistent pulmonary hypertension in the neonate and hepato-renal syndrome. The last infant died 2.2 months after surgery because restrictive cardiomyopathy progressed.
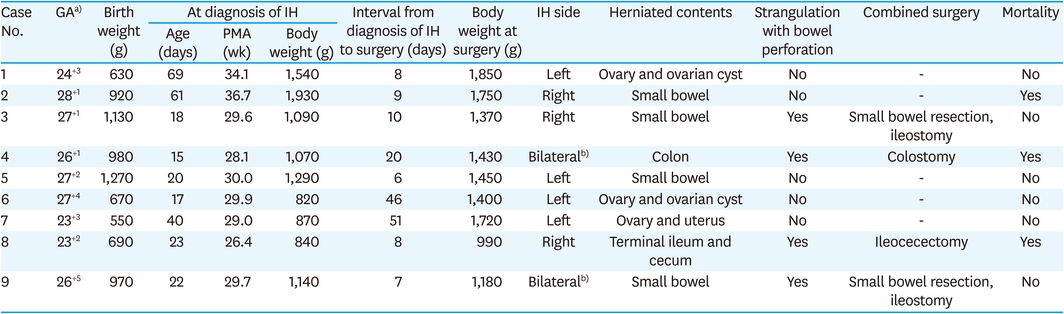
Table 2
Clinical characteristics of incarcerated IH patients
There are some reports about the incidence of incarceration with waiting time from diagnosis to IH surgery. Emergency surgery in those premature infants is associated with a significantly higher incidence of postoperative complications compared with elective repair [8]. Timothy et al. [9] reported that the incarceration rate is lower in premature infants who undergo operative repair during their initial hospitalization (15.7%) than all infants who otherwise undergo IH repair within the first year of life (28.0%). Within the initial hospitalization, the interval from birth to repair has no significant bearing on the risk of incarceration [9]. Wang et al. [10] and Duggan et al. [11] also did not make any conclusive recommendations regarding the optimal timing of repair.
Many pediatric surgeons prefer to perform herniotomy when infants born prematurely reach a certain weight of age [9]. Although this more conservative approach can minimize the risk of surgical and anesthetic complications, it might also increase the risk for incarceration, forcing an emergency procedure with potentially more negative sequelae compared with early elective repair [12, 13]. Timothy et al. [9] reported that delaying repair after 40 weeks post-conceptual age increases the risk of incarceration 2-fold (p<0.001).
In our hospital, the attending physician and nurse in the NICU routinely checked the baby's bilateral groin daily. When the inguinal swelling was palpable, the attending doctor examined, and also ultrasonography was performed. Therefore, the timing of IH diagnosis in our hospital is considered to be accurate. IH was diagnosed at a relatively early age (22 days old and PMA 29.7 weeks) and with low body weight (1,090 g).
According to our policy, we prefer to perform IH repair shortly before the infant's anticipated discharge from the NICU. While planning until elective IH repair before discharge, incarceration occurred median of 9 days after diagnosis of IH (range 6–51 days). Emergency surgery for incarceration was also performed at an earlier age (PMA 31.0 vs. 39.6 weeks) and lower body weight (1,430 vs. 3,021 g) than the results of the previously reported study [8]. Incarceration of 3.8% occurred during our study period (9 of 237). However, it is generally known that the longer the time of uncorrected IH, the higher the possibility of incarceration/strangulation. Incarceration occurred on the median of 9 day after the diagnosis of IH in this study despite a small study case. It may suggest that there are factors influencing the occurrence of incarceration/strangulation other than the duration of uncorrected IH.
All 3 female infants who developed incarceration had genital organ herniation. Strangulation occurred in 4 males only, and in all cases, bowel resection and enterostomy were performed with IH repair.
Our study had some limitations. With its retrospective nature, the selection bias inherent in this study existed. Inadequate data due to the small sample size for this study, making it difficult to analyze the risk factors influencing the study outcome.
In conclusion, this study provided informative data for incarcerated IH in preterm infants successfully treated surgically. Although a small number of cases were involved in this study, close observation is more necessary because the incarceration rate during observation of preterm infants with IH in the NICU is as high as 3.8%. The cause of incarceration was not evaluated because it is not a study comparing IH preterm infants with incarcerated IH. However, further studies analyzing risk factors for incarceration and determining the optimal timing of managing IH in preterm infants may be considered in the future to avoid incarceration.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: L.S., S.J.M.
Data curation: C.K., N.S., B.M.J., K.W.
Formal analysis: B.M.J., K.W.
Funding acquisition: S.J.M.
Investigation: C.K., N.S., K.W., L.S.
Methodology: B.M.J., K.W., L.S.
Project administration: K.W., L.S., S.J.M.
Resources: L.S., S.J.M.
Software: N.S., B.M.J., K.W.
Supervision: L.S., S.J.M.
Validation: L.S.
Visualization: K.W.
Writing - original draft: C.K., N.S.
Writing - review & editing: B.M.J., K.W.
