

Purpose
Thoracoscopic repair of congenital diaphragmatic hernia (CDH) is technically challenging and requires various surgical strategies. However, studies investigating the learning curve of thoracoscopic repair of CDH are rare. The
objective
of this study was to determine whether there is a learning curve of thoracoscopic repair of CDH and analyze its pattern by cumulative sum (CUSUM) analysis.
Methods
From 2008, when the first case was performed, to 2020, children diagnosed with Bochdalek-type CDH who underwent thoracoscopic repair were included. Learning curves of 2 operators were analyzed individually using the CUSUM method which is the running total of differences between operation time of each case and the mean operation time. We divided the CUSUM curve into three phases based on its slope and performed interphase analysis of patients’ baseline characteristics and surgical outcomes.
Results
A total of 111 children (operator A, n=88; operator B, n=23) underwent thoracoscopic repair of CDH during the study period. CUSUM curve of operator A showed an ascending curve from the first case to the 33rd case, then a plateau between the 34th case and the 55th case, and a descending form from the 56th case. In interphase comparisons of surgical outcome of operator A, recurrence rate and rate of complication did not show statistically significant differences. The learning curve of operator B showed a flat overall appearance and plateaued after the 14th case.
Conclusion
Surgical experience based on 33 cases was needed to reach the learning curve to perform thoracoscopic repair of CDH. For a new surgeon experienced with assisting a skilled operator, a relatively high proficiency was obtained from the start with a shorter learning curve. Interphase analysis of surgical outcome suggests that thoracoscopic repair of CDH can be performed without compromising patients’ safety even before reaching the learning curve.
Thoracoscopic repair of congenital diaphragmatic hernia (CDH) is technically challenging and requires various surgical strategies. However, studies investigating the learning curve of thoracoscopic repair of CDH are rare. The objective of this study was to determine whether there is a learning curve of thoracoscopic repair of CDH and analyze its pattern by cumulative sum (CUSUM) analysis.
From 2008, when the first case was performed, to 2020, children diagnosed with Bochdalek-type CDH who underwent thoracoscopic repair were included. Learning curves of 2 operators were analyzed individually using the CUSUM method which is the running total of differences between operation time of each case and the mean operation time. We divided the CUSUM curve into three phases based on its slope and performed interphase analysis of patients’ baseline characteristics and surgical outcomes.
A total of 111 children (operator A, n=88; operator B, n=23) underwent thoracoscopic repair of CDH during the study period. CUSUM curve of operator A showed an ascending curve from the first case to the 33rd case, then a plateau between the 34th case and the 55th case, and a descending form from the 56th case. In interphase comparisons of surgical outcome of operator A, recurrence rate and rate of complication did not show statistically significant differences. The learning curve of operator B showed a flat overall appearance and plateaued after the 14th case.
Surgical experience based on 33 cases was needed to reach the learning curve to perform thoracoscopic repair of CDH. For a new surgeon experienced with assisting a skilled operator, a relatively high proficiency was obtained from the start with a shorter learning curve. Interphase analysis of surgical outcome suggests that thoracoscopic repair of CDH can be performed without compromising patients’ safety even before reaching the learning curve.
As minimally invasive surgery (MIS) was gradually actively performed in pediatric surgery, it began to be applied to the repair of congenital diaphragmatic hernia (CDH). In 1995, the first cases of both thoracoscopic and laparoscopic repair of CDH were reported [1, 2]. Advantages of thoracoscopic repair of CDH include straightforward reduction of herniated organs aided by carbon dioxide (CO2) insufflation, unobstructed view with adequate working space [3], and cosmetic benefits. However, a thoracoscopic repair can be performed only in selected patients due to the risk of intraoperative hypercapnia and acidosis caused by CO2 insufflation to the cardiopulmonary system and a higher recurrence rate compared to an open technique [4]. According to the Korean Association of Pediatric Surgeons survey in 2014, MIS was performed in 29.6% of CDH cases regarding this circumstances [5].
Thoracoscopic repair of CDH is technically challenging and requires various surgical strategies. Tension dispersal is required to reduce the risk of recurrence. And rib fixation or prosthetic patches are needed in certain cases. Also, suturing is difficult due to the lack of wrist articulation of thoracoscopic repair. In addition to the difficulty of the operation itself, it is not easy to improve the skill level due to the rarity of CDH.
These characteristics of thoracoscopic repair of CDH lead to a question of its learning curve. However, studies investigating the learning curve of thoracoscopic repair of CDH are rare, compared with many studies involving thoracoscopic repair of esophageal atresia and tracheoesophageal fistula (EA/TEF), which was initiated after thoracoscopic repair of CDH [1, 2, 6]. Therefore, the objective of this study was to determine whether there is a learning curve of thoracoscopic repair of CDH and analyze its pattern by cumulative sum (CUSUM) analysis frequently used to analyze learning curves of other medical techniques [7, 8, 9].
From August 2008, when the first thoracoscopic repair was performed, to December 2020, all children diagnosed with Bochdalek-type CDH who underwent thoracoscopic repair at a tertiary children’s hospital were included in this study. Contraindication of thoracoscopic repair included high-frequency oscillatory ventilation, extracorporeal membrane oxygenation, severe pulmonary hypertension requiring nitric oxide inhalation, and high suspicion for bilateral defect or type D on chest X-ray or ultrasonography according to the Congenital Diaphragmatic Hernia Study Group (CDHSG) staging system [10].
Two operators performed surgeries in the same following manner. The patient was placed in a lateral decubitus position on the contralateral side of the defect side under general anesthesia. Three trocars were used for the thoracoscope. The first camera trocar was inserted just below the scapular tip. Two working ports were inserted in the fifth or sixth intercostal space in the anterior-posterior axillary line forming a wide angle with each other. CO2 insufflation was slowly injected at a flow rate of 1–2 mL/min until the intrathoracic pressure reached 5 mmHg. If it was challenging to reduce the herniated organs at that pressure, the pressure was increased to 7–8 mmHg while monitoring the cardiopulmonary index. The herniated organs were carefully reduced toward the abdominal cavity using atraumatic graspers. Then, the diaphragmatic muscle and defect were checked. For defects that could be repaired as primary, an interrupted suture was performed using a non-absorbable braided suture (e.g., Ethibond®) and a knot pusher. A diaphragmatic rim was fixed to the rib for a lateral chest wall without muscular rim. In the case of a large defect requiring a prosthetic mesh, primary repair was performed on the medial side of the defect to a level where tension was not severe. The patch was then designed with a size sufficient to create an adequate contact surface between the muscle and the patch. It was inserted through a working port incision and interrupted sutures were then performed. When the hernia sac was present in both primary and patch repair, the hernia sac was plicated on the abdominal side and fixed with the diaphragm or patch simultaneously to prevent recurrence.
Learning curves of operator A and operator B were analyzed using the CUSUM method which is the running total of differences between individual data points and the mean of all data points for quantitative learning curve assessment [9]. In this study, operations performed by each operator were arranged in the order of the date of operation. The first CUSUM was the time taken for the operation minus the mean operation time. The second CUSUM was performed by repeating the method of calculating the sum of the first CUSUM and the value obtained by subtracting the mean operation time from the second operation time. The value of the N-th CUSUM was the sum of the (N-1)-th CUSUM value and the N-th operation time minus the mean operation time. The slope of this CUSUM curve indicated the learning performance trend. The portion showing gentle stabilization of the slope was interpreted as the point of learning curve breakthrough [11].
In each CUSUM curve, the rising section of the curve, the section reaching the plateau, and the falling section were considered as phase 1, phase 2, and phase 3, respectively. Interphase analysis of patients’ baseline characteristics and surgical outcomes was performed. The size of the defect was classified into A, B, C, and D according to the CDHSG staging system [10]. Pearson’s chi-squared test, Fisher's exact test, or Kruskal-Wallis test were used as appropriate, and statistical analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
A total of 111 children (operator A, n=88; operator B, n=23) underwent thoracoscopic repair of CDH during the study period. Operator A and operator B started thoracoscopic repair of CDH in August 2008 and April 2013, respectively. CUSUM curve of operator A showed an ascending curve (phase 1) from the first case to the 33rd case, then a plateau (phase 2) between the 34th case and the 55th case, and a descending form (phase 3) from the 56th case (Fig. 1). The learning curve of operator B had an upward curve (phase 1) with a smaller slope compared to that of operator A, showing an overall flat appearance. It plateaued after the 14th case and did not show an apparent downward curve until the last case (Fig. 2).
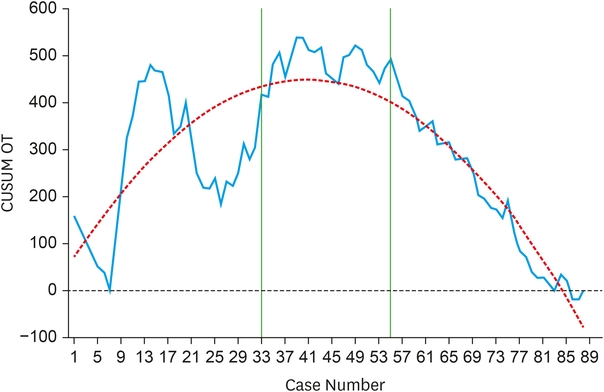
Fig. 1
CUSUM curve of thoracoscopic repair of congenital diaphragmatic hernia of operator A. Blue solid line represents the CUSUM curve based on OT. Orange dotted line represents the curve of the best fit for the CUSUM curve. Green lines indicates breakthrough points of the learning curve [y = 55.6722 + 19.3565 × (Case Number) − 0.2374 × (Case Number)2; Adjusted R2 = 0.7265].
CUSUM, cumulative sum; OT, operation time.
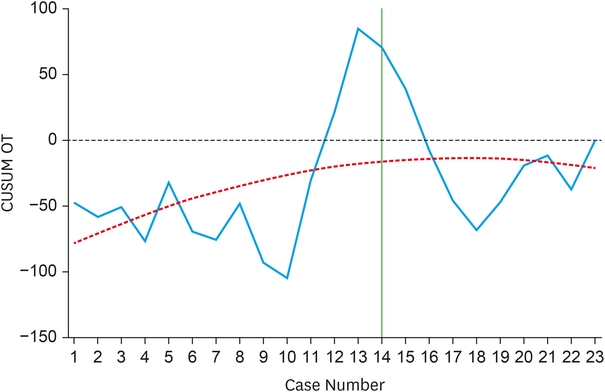
Fig. 2
CUSUM curve of thoracoscopic repair of congenital diaphragmatic hernia of operator B. Blue solid line represents the CUSUM curve based on OT. Orange dotted line represents the curve of the best fit for the CUSUM curve. Green lines indicates breakthrough points of the learning curve [y = −86.1005 + 8.3767 × (Case Number) − 0.2414 × (Case Number)2; Adjusted R2 = 0.0872].
CUSUM, cumulative sum; OT, operation time.
Based on the above results, baseline clinical characteristics were compared for each phase in the learning curve of operator A (Table 1). There were no significant differences in age or weight at the time of surgery of each patient. CDHSG type B and left side defects were most common in all phases. The patch application rate decreased by 24.2% in phase 1, 13.6% in phase 2, and 6.1% in phase 3, which was not statistically significant (p=0.107).
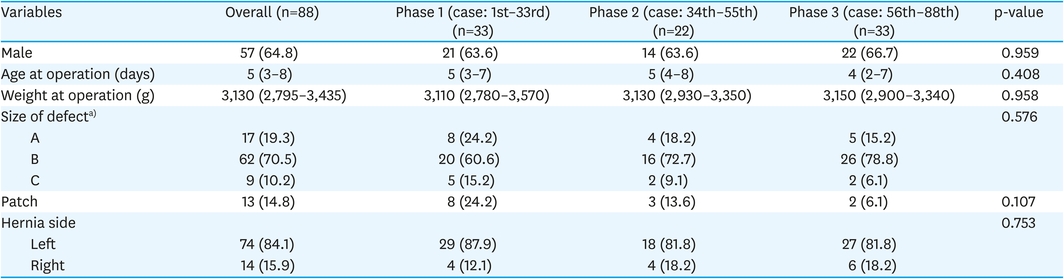
Table 1
Interphase comparisons of patients' baseline clinical characteristics of operator A
In interphase comparisons of surgical outcome of operator A (Table 2), the median operation time was similar with differences between all phases occurring within 10 minutes (p=0.074). The recurrence rate decreased from 27.3% in phases 1 and 2 to 18.2% in phase 3 (p=0.626). Open conversion was not observed in any phase. Time to full feeding, in-hospital recurrence rate, and rate of complication (Clavien-Dindo classification (CDC) grade 3 or higher) did not show significant differences between phases. However, the length of hospital stay was 15 days postoperatively in phase 1 which was the shortest among the three phases (p=0.010).

Table 2
Interphase comparisons of intraoperative parameters and surgical outcome of operator A
Interphase comparison of baseline clinical characteristics of operator B also showed no significant differences (Table 3). Patients with CDHSG type B was 78.6% in phase 1 and 77.8% in phase 2 (p=0.926). Patch application rate in each phase was 14.3% and 11.1% (p=1.0). There was no significant difference in operation time and postoperative outcome between phases of operator B (Table 4). Recurrence rate and rate of complication (CDC grade 3 or higher) were both higher in phase 1 without statistical significance.
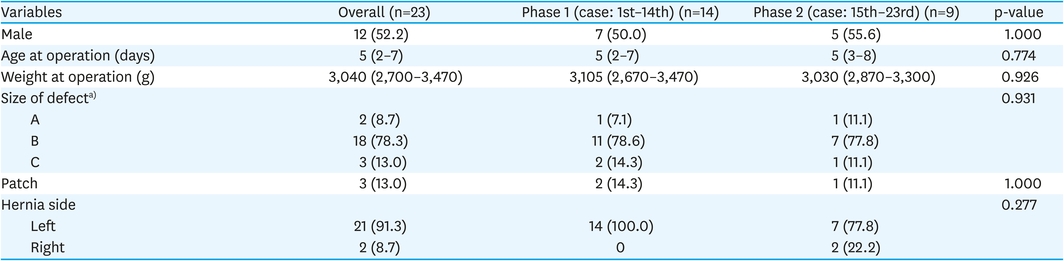
Table 3
Interphase comparisons of patients' baseline clinical characteristics of operator B

Table 4
Interphase comparisons of intraoperative parameters and surgical outcome of operator B
Thoracoscopic repair of CDH is actively performed in many children’s hospitals, although its detailed indications can vary in each hospital. However, no studies reporting the learning curve associated with this surgical approach have been done to the best of our knowledge. Therefore, we analyzed learning curves of thoracoscopic repair of CDH performed by 2 operators using the CUSUM method. And surgical outcomes were analyzed for each phase of the learning curve. As a result of a quantitative assessment using the running total of differences in the operative time of each case and the mean operative time of all cases, we found that the learning curve for thoracoscopic repair of CDH showed three different trends of slope, a positive slope, a plateau, and a negative slope. Based on this finding, we could divide the learning curve into three phases similar to that of robotic-assisted laparoscopic colorectal surgery [9] and vacuum-assisted breast biopsy [12]. The positive slope of phase 1 represents the learning period; the plateau (phase 2) represents the period of accumulating additional skills and experiences; and the negative slope of phase 3 means the mastery period.
The learning curve of operator A was analyzed based on a total of 88 cases. The breakthrough of the learning curve started when it reached a plateau after the 33rd case (Fig. 1). The descending curve starting from the 56th case was interpreted as the point of decrease in the operation time due to acquisition of the surgical skills. Since there was no published study involving the learning curve of thoracoscopic repair of CDH, it was impossible to directly compare the number of cases required to reach the plateau phase. However, compared with the study of Kim et al. [13], which plateaued in the 10th case for thoracoscopic repair of esophageal atresia and distal tracheoesophageal fistula (EA/dTEF), the number of cases required to break the learning curve of thoracoscopic repair of CDH was relatively large. Compared with Kim's study that investigated EA/dTEF exclusively, the CDH in this study involved diverse surgical cases, and thus the various surgical techniques and strategies might have contributed to a longer learning curve. There was no significant difference in the defect size and patch use between the phases of operator A (Table 1). However, various surgical strategies were required during each surgery, even for the same type of defect, such as rib fixation in the absence of posterolateral diaphragmatic rim, the direction of repair to minimize the tension, and the range of patch application. In addition, a direct comparison of the present study might not be accurate, because Kim's study used a binary outcome measure considering that the case with operative time shorter than the mean operative time was a failure and the opposite case was a success.
In the surgical outcome of operator A, the recurrence rate before the breakthrough of the learning curve was higher than that in phase 3, although the difference was not statistically significant (Table 2). Thus, thoracoscopic repair can be performed safely without the higher risk of recurrence even before a learning curve breakthrough. Similarly, rates of complications with CDC grade 3 or higher were 30.3% and 31.8% in phase 1 and phase 2, respectively, higher than that (18.2%) in phase 3. Such decrease in the incidence of complications as the number of cases increases can be regarded as another evidence for a learning curve [12, 14]. The difference in complication rates between phases was also not statistically significant. Thus, thoracoscopic repair can be performed without the risk of significant complications even before the learning curve is reached.
The learning curve of operator B was relatively flat without apparent decline, which suggests proficiency from the beginning. It plateaued after the 14th case when 33 cases were required for operator A (Figs. 1 and 2). It did not show a pattern that could be divided into three phases like that of operator A. However, it shared the ascending and plateau pattern of phase 1 and phase 2 of operator A. This means operator B have reached his learning curve but not his mastery phase during the study period. Shorter learning curve and initial proficiency of operator B despite similar patients’ preoperative status to those of operator A are attributed to experience assisting or observing surgeries performed by operator A before conducting surgeries independently. During this training period, the trainee could have accumulated the surgical know-how and strategies of operator A. These results suggest that a pediatric surgeon can be trained effectively by indirectly experiencing or observing the operations conducted by an experienced pediatric surgeon.
In this regard, Kim et al. [13] interpreted that practical tips related to techniques provided by an experienced operator, and a surgical protocol reduced the trainee’s learning curve associated with thoracoscopic repair of EA/TEF. Based on the current trend of declining birth rates in Korea (0.837 in 2020), pediatric surgeons take longer to improve their surgical skills due to fewer surgical cases. Under these circumstances, establishing a quality control protocol and active sharing of cases at each hospital and between pediatric surgeons can help nurture surgical competency. A hands-on training program currently run by Korean Association of Pediatric Surgeons would also help pediatric surgeons shorten their learning curves.
This study has some limitations. First, it was impossible to compare the learning curves between operators exposed to a similar number of cases. Second, since there was no existing study to refer to, the number of cases required to reach the learning curve could not be generalized. The study results will be compared when the number of cases of operator B increases further, and the learning curves of other operators are shared. However, based on quantitative assessment using the CUSUM technique, we distinguished the three phases of the learning curve and compared the surgical outcomes between different phases.
In conclusion, in this study using the CUSUM technique, we found that surgical experience based on 33 cases was needed to reach the learning curve by the operator to perform thoracoscopic repair of CDH. However, the interphase comparisons of recurrence rate and complications did not show statistically significant differences. Thus, it seems that thoracoscopic repair of CDH can be performed without compromising patients’ safety even before reaching the learning curve. However, in the case of a new surgeon experienced with assisting a skilled operator during surgery, a relatively high proficiency was obtained from the start with a shorter learning curve and a plateau reached after 14 cases. Therefore, an experienced operator is needed for guidance during the learning curve period, underscoring the importance of assisting and observing surgeries performed by an experienced operator.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.H., N.J.M.
Data curation: H.S.W., H.S.
Formal analysis: K.H.
Investigation: K.H.
Methodology: K.H., N.J.M.
Writing - original draft: H.S.W., K.H.
Writing - review & editing: H.S.W., K.H.
