
 , Hyunhee Kwon
, Jueun Park
, Dae Yeon Kim
, Hyunhee Kwon
, Jueun Park
, Dae Yeon Kim

Purpose
The International Society for the Study of Vascular Anomalies (ISSVA) classification is crucial in diagnosing vascular anomalies (VAs), surpassing the International Classification of Diseases 10th Revision. This study aims to reevaluate diagnoses using ISSVA criteria and explore diagnostic patterns.
Methods
Analyzing 138 pediatric VA patients diagnosed via magnetic resonance imaging from 2018 to 2023 at Asan Medical Center, we reviewed clinical, imaging, pathology, and genetic data. Diagnoses were revised per 2018 ISSVA criteria, assessing discrepancies.
Results
Among 133 VA cases, 125 were malformations and eight were tumors, mostly in the head and neck. Clinical and imaging diagnoses disagreed in 51 cases. Some initially complex malformations were simplified. Lymphatic malformation cases shifted to VAs and vascular tumors were identified post-initial diagnosis.
Conclusion
Accurate diagnosis of VAs is essential for prognosis, treatment planning, and predicting outcomes. However, 14.2% of patients showed discordance between clinical diagnoses and imaging findings. Capillary malformations were often overlooked in imaging but became evident with relevant clinical findings. Adopting a multidisciplinary approach and a unified diagnosis based on ISSVA classification is crucial for clearly defining VAs.
The International Society for the Study of Vascular Anomalies (ISSVA) classification is crucial in diagnosing vascular anomalies (VAs), surpassing the International Classification of Diseases 10th Revision. This study aims to reevaluate diagnoses using ISSVA criteria and explore diagnostic patterns.
Analyzing 138 pediatric VA patients diagnosed via magnetic resonance imaging from 2018 to 2023 at Asan Medical Center, we reviewed clinical, imaging, pathology, and genetic data. Diagnoses were revised per 2018 ISSVA criteria, assessing discrepancies.
Among 133 VA cases, 125 were malformations and eight were tumors, mostly in the head and neck. Clinical and imaging diagnoses disagreed in 51 cases. Some initially complex malformations were simplified. Lymphatic malformation cases shifted to VAs and vascular tumors were identified post-initial diagnosis.
Accurate diagnosis of VAs is essential for prognosis, treatment planning, and predicting outcomes. However, 14.2% of patients showed discordance between clinical diagnoses and imaging findings. Capillary malformations were often overlooked in imaging but became evident with relevant clinical findings. Adopting a multidisciplinary approach and a unified diagnosis based on ISSVA classification is crucial for clearly defining VAs.
Vascular anomalies (VAs) are defined as structural abnormalities of the vasculature, occurring during vasculogenesis, angiogenesis, and lymphangiogenesis [1]. They include deformities across superficial and deep structures of the body. Because of their overlapping characteristics, it is very difficult to identify each disease from another. However, distinguishing each disease is important for understanding the disease and establishing a treatment plan. Recently, VAs have been divided into vascular tumors and malformations [2]. Vascular tumors are classified according to the degree of malignancy.
Vascular malformation is classified according to the characteristics of the vessels involved. The classification of Congenital Lipomatous Overgrowth, Epidermal Nevis, Spinal/Skeletal Anomalies/Scoliosis (CLOVES) syndromes has been systematically developed since its first classification in 1982 [3]. Initially, it reflected the developmental characteristics and the characteristics of the structures and lesions involved in the visual lesion-oriented criteria. In the 2018 edition of the International Society for the Study of VAs (ISSVA) classification, which is widely employed nowadays, it embraced the description of several diseases that were previously unclassified. Various diagnostic imaging techniques such as computed tomography, doppler ultrasound, and angiography have been utilized for diagnosing and characterizing CLOVES syndromes in detail. However, among these methods, magnetic resonance imaging (MRI) stands out as the preferred modality due to its superior ability to visualize soft tissue lesions.
Therefore, in this study, we re-classified diagnoses of our patients diagnosed and treated for VAs at our department (Department of Pediatric Surgery, Asan Medical Center) following the ISSVA classification. The purpose of this reclassification was two-fold: firstly, to formulate a treatment plan grounded in accurate diagnoses, and secondly, to enhance communication during the multidisciplinary approach. Additionally, we aimed to pave the way for the future implementation of precision medicine through the outcomes of this research.
This study was designed as a retrospective single-center study. We reviewed the medical records of 138 patients diagnosed and followed up for VA between 2018 and 2023 in pediatric surgery at Asan Medical Center in Seoul, Republic of Korea (Fig. 1, Institutional Review Board approval ID: A20232572). The diagnoses in this study relied on the 2018 revised ISSVA classification for VAs. Only patients with available MRI images were considered, resulting in the inclusion of 138 out of 149 patients in the final analysis. Patients without MRI images (n=8) or those lacking MRI images at the time of initial diagnosis (n=3) were excluded from our study. Informed consent was waived due to the retrospective nature of the study. The photographs were taken with the consent of the child and the guardian for clinical purposes, and were used after notifying them of the use in the study and obtaining their consent. The photos were used after removing all information that could identify the patient. Statistical analysis was performed using IBM SPSS Statistics version 21 (IBM Corp., Armonk, NY, USA). Continuous variables are expressed as either mean±standard deviation or range, as specified. Categorical variables are presented as frequencies and percentages. A p-value less than 0.05 was deemed statistically significant, indicating a significant result.
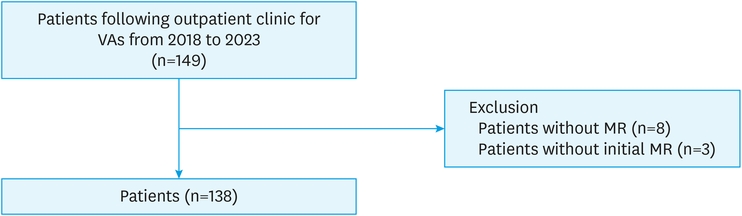
Fig. 1
The flow of our patient population. A total of 149 patients diagnosed and treated for VAs were identified and selected. Among them, 11 patients were excluded due to a lack of data, and 138 patients were enrolled in our study.
VA, vascular anomaly; MR, magnetic resonance.
The sex ratio of the children who took part in this study was equal, indicating an equal representation of both males and females (Table 1). The age of the participants exhibited a broad distribution, with a mean of 110.35 months and a large standard deviation of 956.31 months. This wide age range was due to the inclusion of adult patients who visited our department with VAs.

Table 1
Patient characteristics (n=138)
We conducted a reclassification of the diagnosis of our patients based on pre-treatment MRI images, following the ISSVA classification (Fig. 2). Out of the 138 patients included in the analysis, 133 were definitively identified as having VAs. Among these, 125 patients were diagnosed with CLOVES syndromes, with the majority (122 cases) being slow-flow malformations, and the remaining three cases were classified as fast-flow malformations. Furthermore, there were only eight patients diagnosed with vascular tumors in the study cohort.
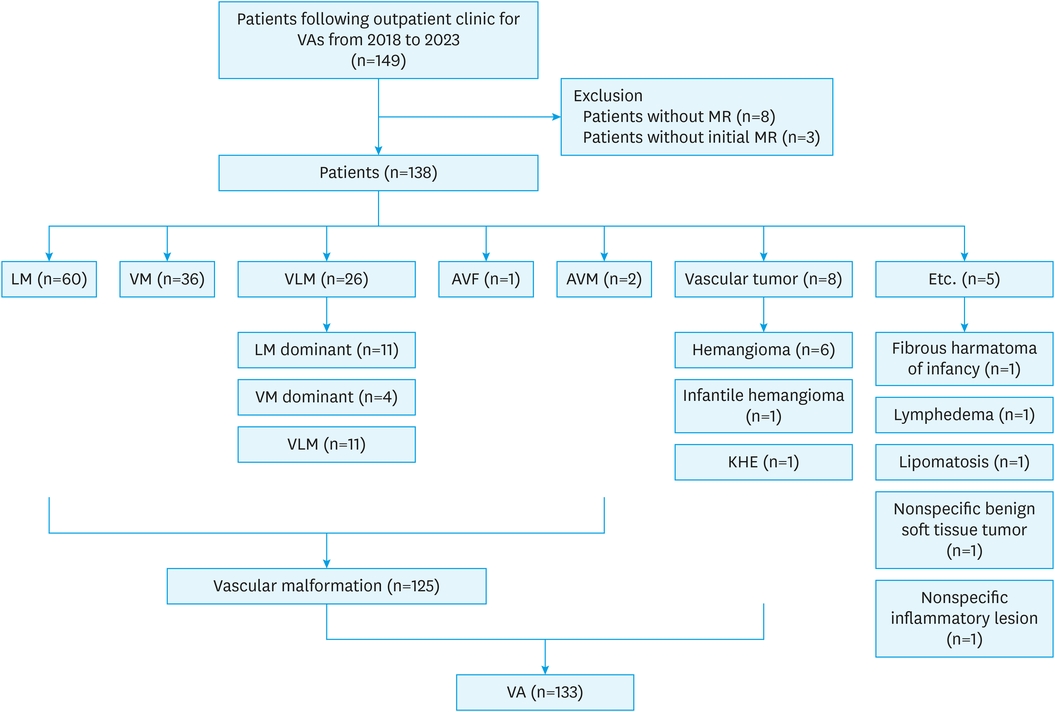
Fig. 2
Re-classification of patients by ISSVA classification for VAs©. We re-classified the initial diagnosis of our patients depending on the 2018 ISSVA classification for VAs©, the most recently revised version (May 2018). In 133 patients, vascular anomaly was diagnosed, and CLOVES syndrome was identified in 125 patients. We put each disease in a detailed, specific disease nomenclature. The incidence of vascular tumors was relatively low in our study population.
VA, vascular anomaly; MR, magnetic resonance; LM, lymphatic malformation; VM, venous malformation; VLM, venolymphatic malformation; AVF, arteriovenous fistula; AVM, arteriovenous malformation; KHE, kaposiform hemangioendothelioma; ISSVA, International Society for the Study of Vascular Anomalies; CLOVES, Congenital Lipomatous Overgrowth, Epidermal Nevis, Spinal/Skeletal Anomalies/Scoliosis.
Out of the 133 patients with unequivocal VAs in the study, a total of nine patients were found to have accompanying syndromes known to be related (Table 2). Among these cases, six patients received a clinical diagnosis, while four patients had their syndromes confirmed through genetic testing. The most frequently observed syndrome was CLOVES syndrome, followed by Klippel-Trénaunay syndrome. Except for patient six, the lesions were observed to spread across multiple parts of the body in the remaining patients with VAs (Fig. 3A).
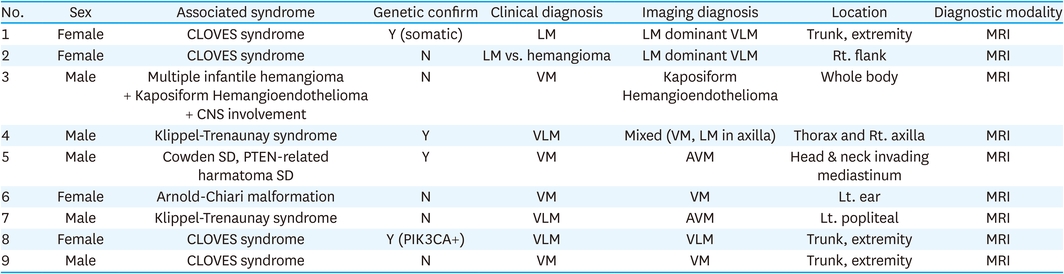
Table 2
Patients suspected of VA-associated syndrome
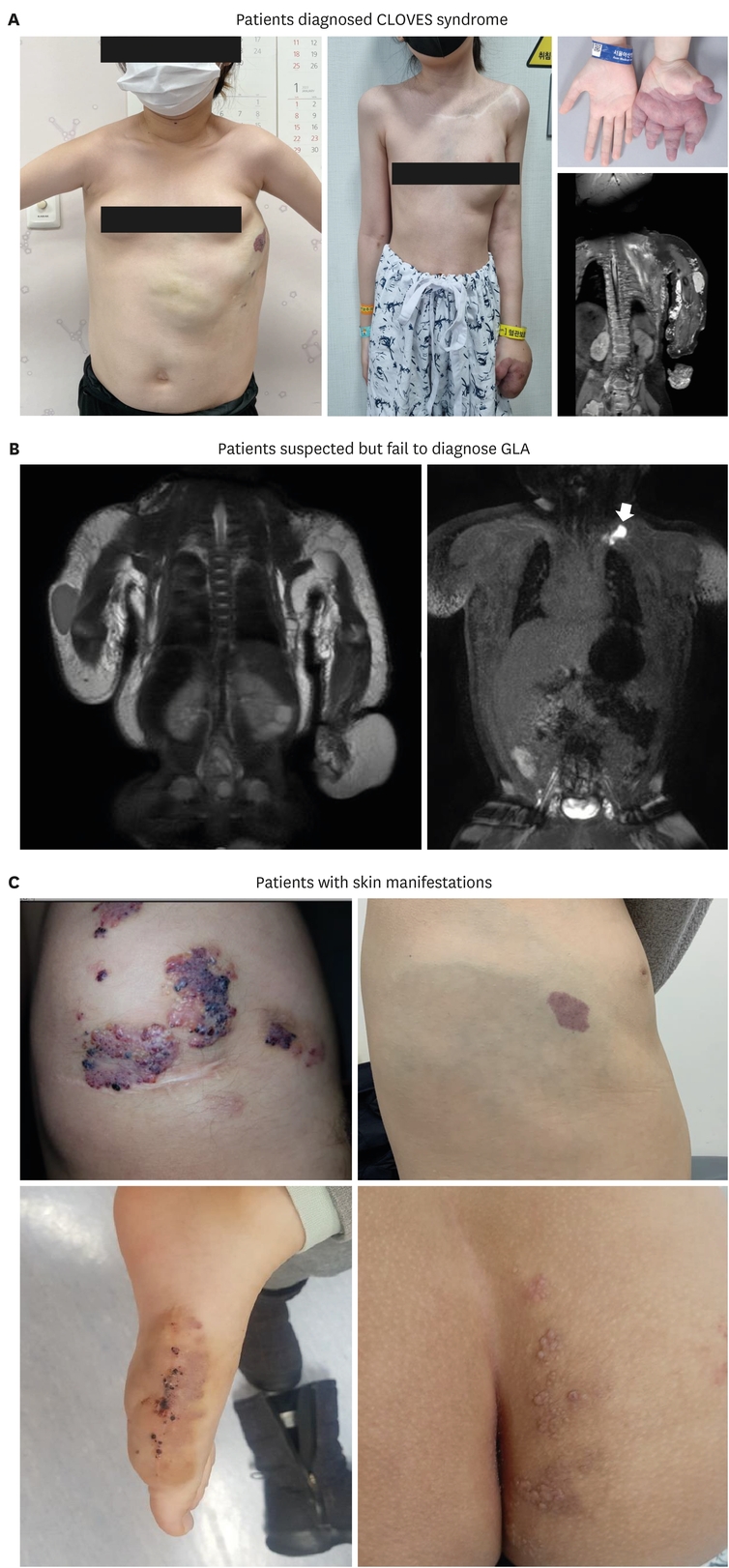
Fig. 3
Patients with various vascular anomalies. (A) Patients diagnosed CLOVES syndrome: clinical photo of two patients diagnosed CLOVES syndrome illustrated. The patient in the left photo showed clinical manifestation of CLOVES syndrome which was confirmed by molecular diagnosis. The patient on the right also showed features and PIK3CA gene mutation was detected. (B) Patients suspected but failed to diagnose GLA: generalized lymphatic malformation and soft tissue hypertrophy were observed in this patient, we proceeded with central lymphangiography during MRI but the connection between the lesion and central lymphatic channel was not identified. (C) Patients with skin manifestations: in 6 patients, skin lesion was identified and recorded in our medical records. It can easily be missed in imaging diagnosis due to small size. Therefore, it is important to keep records, including photos and descriptions, in the medical chart.
CLOVES, Congenital Lipomatous Overgrowth, Vascular Malformations, Epidermal Nevis, Spinal/Skeletal Anomalies/Scoliosis; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; GLA, generalized lymphatic anomaly; MRI, magnetic resonance imaging.
A total of six patients exhibited clinical characteristics consistent with phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA)-related overgrowth spectrum (PROS; Table 3). Among them, patient one had fibro adipose hyperplasia or overgrowth confirmed as a specific subtype. However, for the remaining five patients, it was challenging to subclassify their condition. Gene studies were performed on four patients, and somatic mutations were confirmed in two of them, but not in the other two patients.

Table 3
Patients with PROS
Patient number four in the table was clinically suspected of having generalized lymphatic anomaly. Further work-up, including central lymphangiography and surgical biopsy on the lesion with the molecular diagnosis was performed. However, no somatic mutation in the PIK3CA gene was identified from this specimen. Additionally, magnetic resonance with central lymphangiography revealed that there was no connection between the lesion and central lymphatics (Fig. 3B). In the top left and bottom left photos, vascular malformations of the skin can be observed. Capillary malformation is seen in the top right photo, while the bottom right photo reveals typical skin lesions of lymphatic malformations (LMs).
The diagnosis of VA in our study became more precise and clearer by a combination of visual examination, imaging studies, and histopathological examination in this study. We were able to understand the direction of these diagnostic differences (Table 4). Clinical diagnoses were more intuitive and tended to follow well-known diagnoses, such as venous malformation (VM), LM, arteriovenous fistula, and arteriovenous malformation (AVM). However, after diagnostic imaging, diagnoses advanced towards more detailed and specific ones that reflected the characteristics of the lesion, for example, venolymphatic malformations. Moreover, in some cases, the imaging findings led to completely different diagnoses than what was initially suspected or clinically assumed. This highlights the importance of utilizing various diagnostic modalities and approaches to achieve more accurate and comprehensive diagnoses of VAs.
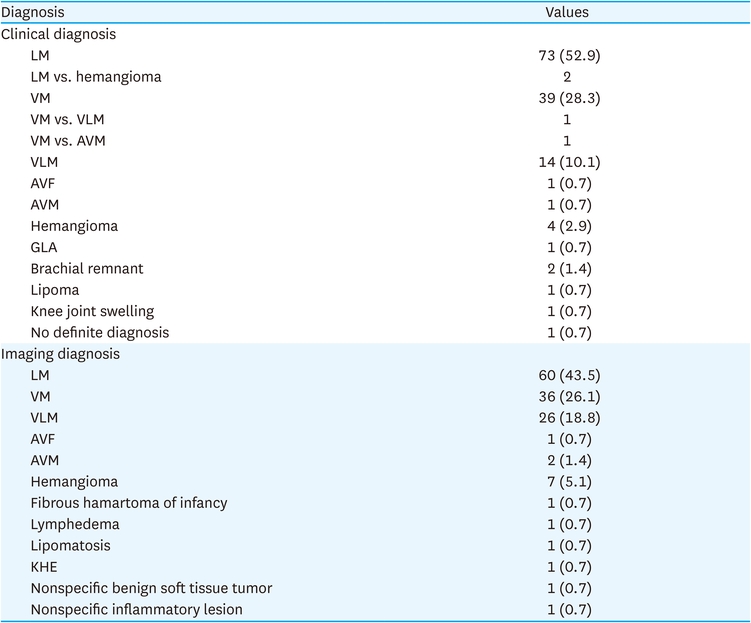
Table 4
Discrepancy between clinical and imaging diagnosis
The detailed characteristics of VM are as follows (Table 5): however, it is important to note that in the case of macrocystic LM, none of the patients exhibited pure macrocystic forms. Instead, most of them were confirmed to have mixed characteristics, indicating the presence of elements from both macrocystic and other types of LM.
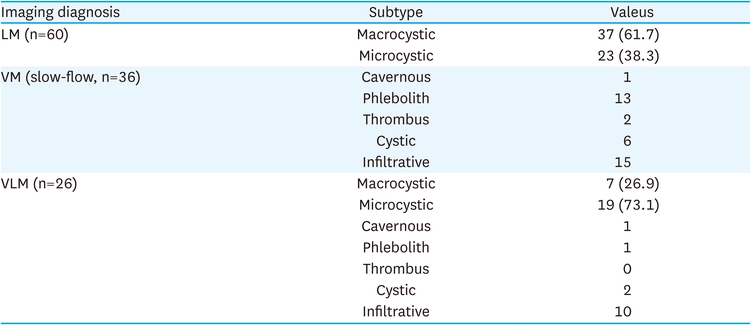
Table 5
Detailed characteristics of VM
In 13 patients, fibro adipose vascular anomaly (FAVA) was diagnosed from MRI. All lesions were identified in the limbs, and nine of them were found in the lower limbs. Most were identified as VMs through imaging studies. However, in three cases, the presence of accompanying LMs was also suspected (Table 6).
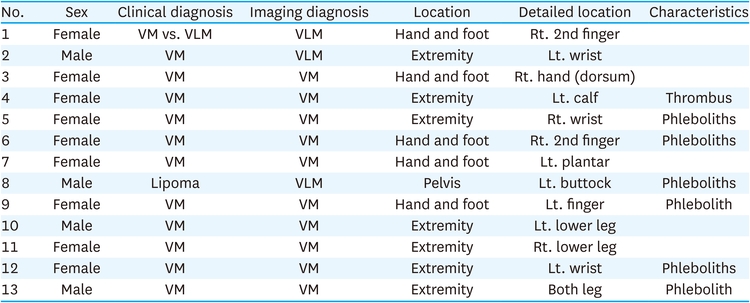
Table 6
New challenge: diagnosing FAVA
The distribution of lesions according to their location is as follows (Fig. 4):
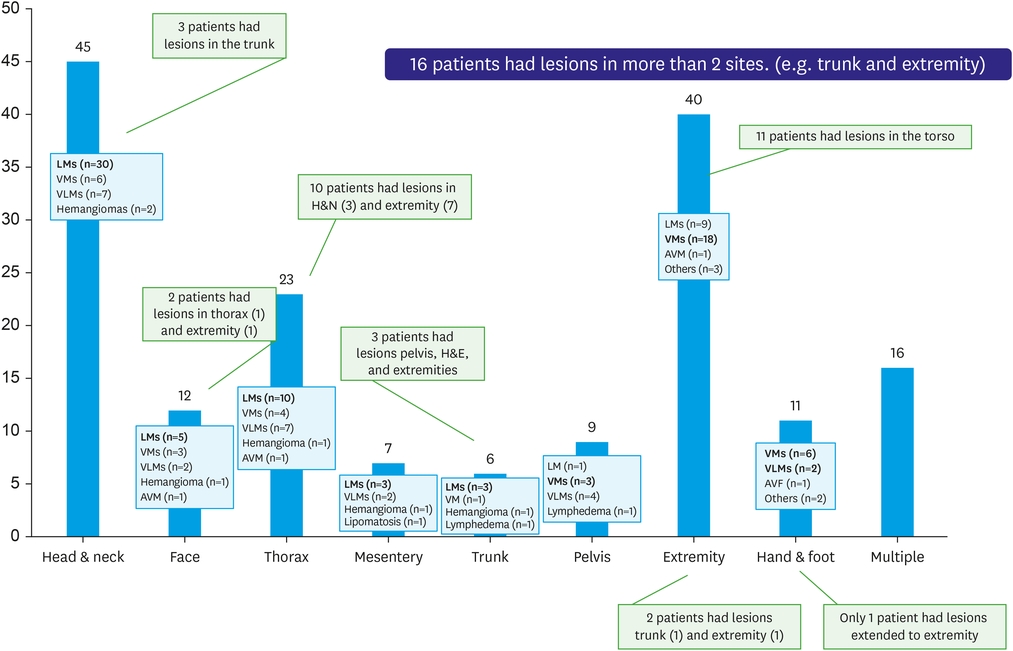
Fig. 4
Vascular anomalies depending on their location. We sought to show differences in diagnosis depending on the location of the lesion. The predominant lesions were different from each body region. Parts of the body where lesions occur frequently were identified in the following order: head and neck, extremities (excluding hands and feet), and thorax. Sixteen patients showed lesions discrete more than two sites of the body.
LM, lymphatic malformation; VM, venous malformation; VLM, venolymphatic malformation; AVM, arteriovenous malformation; AVF, arteriovenous fistula.
Face and head/neck: LM was the predominant type observed in this area. The same trend was observed in the thorax and trunk regions.
Extremities: VM was found to be the dominant type as the lesions progressed towards the extremities.
Multiple sites: in 16 children, the lesions were found to span two or more sites in the body.
Skin lesions were noted as a report that could be easily overlooked in the MRI imaging technique.
Among the patients, six individuals exhibited accompanying skin lesions (Fig. 3C). It was observed that documenting skin manifestations is crucial either during the initial clinical diagnosis or using clinical photographs. This ensures that important information about the skin condition is not missed and contributes to a comprehensive evaluation and diagnosis of VAs.
VA is an old disease, first mentioned as "angiomas" by Virchow [4] in 1863, but diagnosis and treatment have not been fully established. In this aspect, the nomenclature and definition of each disease have still been unclear and confusing. Developments in imaging and molecular diagnosis have enabled us to distinguish each disease from another. Additionally, it has made targeted therapy for each disease possible. The International Classification of Diseases 10th Revision, a standard nomenclature system of disease, did not reflect the rapid evolution of diagnosis. Mulliken and Glowacki’s classification and the Hamburg classification system were also proposed but are not widely used now [1]. The ISSVA classification was first adopted in 1996 and has been updated; it is considered the most up-to-date and comprehensive classification of VA [5]. This is because it reflects clinical, radiological, and histopathologic features and tries to incorporate recent changes in the field of VA [1, 6]. Now it serves as a compass in the VA world for medical professionals specializing in disease management. In the ISSVA classification, proliferative vascular lesions, referred to as "tumors," are differentiated from non-proliferative lesions, referred to as "malformations." Vascular tumors are subdivided into benign, borderline, and malignant categories, and CLOVES syndromes are subdivided into simple, combined, and major named vessels, associated with other anomalies, according to the type of vessels with anomalies [2]. In this study, we performed diagnoses based on MRI imaging and the ISSVA classification. This was compared with the clinical diagnosis. There was a difference between clinical diagnosis and imaging diagnosis, which was thought to reflect the strengths of MRI, which better reflects the characteristics of blood vessels and soft tissues within the lesion. The combination of MRI and ultrasonography helped make a more accurate diagnosis through static and dynamic visualization of the lesion, and the ISSVA classification was found to help clarify the nomenclature [7, 8]. Through this, we were able to approach a correct treatment plan.
Malformations associated with other anomalies are described independently, and these diseases are characterized by CLOVES syndromes accompanied by soft tissue or skeletal anomalies. PROS was added as an appendix and shows symptoms such as segmental overgrowth of the body due to activation by somatic mutation of phosphatidylinositol 3-kinase (PI3K) [9, 10]. The ISSVA classification, updated in 2018, specifies the syndrome associated with CLOVES syndrome, clinical findings that serve as diagnostic criteria, and causative genes. This is meaningful in that it not only reveals and describes the genes that cause the disease, but also specifies a standard diagnosis that can be given. Additionally, we classified the diseases according to the primary site, and through this, we were able to identify the characteristics of VM occurrence in each body part. This is expected to serve as a basis for establishing an imaging diagnosis plan in the clinical diagnosis process through additional research. Finally, we diagnosed FAVA and could establish a treatment strategy more suitable for the disease [11, 12].
Treatment is based on surgical excision and sclerotherapy, and conservative management including ablation, laser, and medical treatment is used in combination depending on the disease. Surgical resection (complete or partial) is the main treatment for VA [13]. According to the principles by Mulliken et al. [14] in 2000, resection should be done by focusing on the anatomical region, minimizing bleeding through a staged approach if necessary, protecting major blood vessels and nerve structures, and applying a closed suction system after surgery. Sclerotherapy is effective when applied to macrocystic or mixed LMs. Radiofrequency ablation, neodymium:yttrium-aluminum-garnet, and cryoablation can be selectively used depending on each disease [11, 15, 16, 17, 18]. For example, there are reports that cryoablation was effective in patients with FAVA [19, 20]. Target agents have become established as treatments for complicated and recurrent VA for which there are no other treatment options [21, 22]. Activating mutations in the PI3K gene are a major pathway in the pathogenesis of VA and are important because many currently commonly used targeting agents target the PIK3CA/Akt/mTOR pathway. The signal via the Tie2/VEGFR3 receptor, PI3K, Akt, and mTOR acts to cause cell proliferation [23, 24, 25]. Sirolimus is a representative drug that acts on mTOR, and alpelisib is a representative drug that acts on PI3K. In addition, various targeting agents targeting molecules of the PIK3CA/Akt/mTOR and RAS/MEK/ERK pathways are being developed or are in clinical trials. Pazopanib for VEGFR, miransertib for Akt in PROS, vemurafenib for BRAF in AVM, and trametinib for MEK in AVM are among them. Classification of VA according to the ISSVA classification provides a rationale for determining treatment policies [26]. As the characteristics of each disease are reflected, the classified diseases provide a basis for what kind of treatment to administer. Additionally, it has the advantage of providing information on gene mutations for each disease, which is the basis for selecting a target agent. In this study, we confirmed the diagnosis based on the ISSVA classification in patients for whom molecular diagnosis was attempted. An association with the syndrome was confirmed in 9 patients included in this study, but only 4 patients underwent genetic testing. This suggests that considering the characteristics of these patients showing lesions throughout the body, genetic testing should be performed in preparation for future targeted therapy.
The limitation of our study is that it focused exclusively on patients with visible mass-like lesions, such as slow-flow malformations, who sought treatment at our department. In contrast, the incidence of vascular tumors was relatively low in our study population. This narrow scope may not fully represent the entire spectrum of CLOVES syndromes, which encompass diverse manifestations requiring a multidisciplinary approach. Furthermore, the lack of utilization of pathological and molecular biological diagnoses through histological examination could be viewed as a critical aspect to consider for future improvements in the diagnostic process. Incorporating these diagnostic techniques may enhance the overall diagnostic accuracy and provide a more comprehensive understanding of VAs.
Accurate diagnosis of VA is important in predicting the course of the disease, treatment policy, and effect. In 14.2% of patients, imaging diagnosis results did not match the clinical diagnosis. Considering that VA is a heterogeneous group of diseases, it is difficult to derive an accurate diagnosis solely based on clinical impressions. In the same context, to incorporate the rapidly advancing treatment approaches, it is evident that diverse diagnostic methods, including imaging, are necessary. Also, capillary malformations (n=6) tended not to be included in the reading of imaging tests, so a description of skin lesions should be included during clinical diagnosis. Establishing a diagnostic procedure including various diagnostic approaches that can clarify the diagnosis based on the ISSVA classification and a multidisciplinary approach is considered important for accurate diagnosis and proper management of VAs.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.D.Y.
Data curation: G.S.
Formal analysis: G.S.
Supervision: K.D.Y.
Visualization: K.D.Y., G.S.
Writing - original draft: G.S.
Writing - review & editing: G.S., K.H., P.J., K.D.Y.
