
 , Ki-Yun Lim
, Keehoon Hyun
, Heecheol Chang
, Ki-Yun Lim
, Keehoon Hyun
, Heecheol Chang

Purpose
Crohn’s disease (CD) is mainly presenting gastrointestinal symptoms but also may involve perianal diseases, with anal fistula being the most common. Anal fistula surgery performed without recognition that the patient has CD increases the complications such as delayed wound healing and anal sphincter injury. This study aimed to investigate clinical symptoms and surgical findings that could allow early diagnosis of CD in patients aged 10 to 19 years who underwent anal fistula surgery.
Methods
Among the 320 patients under the age of 19 who underwent anal fistula surgery, those who were diagnosed with tuberculosis fistula were excluded, medical records of 316 patients were examined. We investigated the characteristics of anal fistula and postoperative wounds as well as the colonoscopic and surgical findings.
Results
Compared to 272 patients not diagnosed with CD (non-CD group), 44 patients diagnosed with CD (CD group) showed significantly higher levels of C-reactive protein as well as anal discharge, family history of inflammatory bowel disease, history of anal fistula, diarrhea, abdominal pain, weight loss, complex anal fistula, recurred anal fistula, delayed wound healing and friable/edematous/granulation of surgical site.
Conclusion
For patients aged 10–19 years with anal fistulas, emphasizing early suspicion and an active diagnostic work-up is essential for early diagnosis of CD.
Crohn’s disease (CD) is mainly presenting gastrointestinal symptoms but also may involve perianal diseases, with anal fistula being the most common. Anal fistula surgery performed without recognition that the patient has CD increases the complications such as delayed wound healing and anal sphincter injury. This study aimed to investigate clinical symptoms and surgical findings that could allow early diagnosis of CD in patients aged 10 to 19 years who underwent anal fistula surgery.
Among the 320 patients under the age of 19 who underwent anal fistula surgery, those who were diagnosed with tuberculosis fistula were excluded, medical records of 316 patients were examined. We investigated the characteristics of anal fistula and postoperative wounds as well as the colonoscopic and surgical findings.
Compared to 272 patients not diagnosed with CD (non-CD group), 44 patients diagnosed with CD (CD group) showed significantly higher levels of C-reactive protein as well as anal discharge, family history of inflammatory bowel disease, history of anal fistula, diarrhea, abdominal pain, weight loss, complex anal fistula, recurred anal fistula, delayed wound healing and friable/edematous/granulation of surgical site.
For patients aged 10–19 years with anal fistulas, emphasizing early suspicion and an active diagnostic work-up is essential for early diagnosis of CD.
Crohn’s disease (CD) is a chronic idiopathic inflammatory disease presenting gastrointestinal symptoms and may also cause extraintestinal symptoms, including skin, joint, and eye problems; fatigue; and weight loss [1]. Although CD can affect any part of the gastrointestinal tract, it usually affects terminal ileum and colon. CD symptoms, including abdominal pain, fever, diarrhea, blood- or mucus-containing stools, and clinical signs of intestinal strictures, occur with a recurrent cycle of flare-ups and remission [2]. Moreover, 10%–80% of patients with CD present symptomatic anal diseases, with anal fistula being the most common, followed by perianal abscesses, anal fissure, anal skin tags, rectal strictures, and hemorrhoids [3, 4, 5, 6, 7, 8]. Additionally, 10%–45% of patients present anal lesions as the initial CD symptom [3, 9, 10, 11]. Among them, 17.2% are diagnosed with CD more than 6 months after the initial manifestation of anal lesions, while 26.9% present anal lesions within 6 months of CD diagnosis [4].
Since the first description of anal fistula as a complication of local ileitis in patients with CD in 1938 [12], several diagnostic and therapeutic approaches have been developed. Following the development of biologic agents, a combination of medical and surgical treatments for anal fistulas in patients with CD is recommended by the European Crohn and Colitis Organization guidelines [13, 14]. Infliximab is the first-line treatment; moreover, a multidisciplinary approach is the standard therapy for anal fistula in patients with CD [8, 15, 16, 17]. Among patients with CD, those with anal fistula have worse disease progression than those without anal fistula [18, 19]. Since early diagnosis of CD in patients with anal fistula can effectively improve their prognosis, it is important to assess the risk of CD at the diagnosis of anal fistula in order to inform therapeutic approaches and prognosis.
According to recent Korean studies on inflammatory bowel disease (IBD) [20], the standardized prevalence of CD increased by 1.9 times, from 15.9/100,000 persons in 2009 to 29.6/100,000 persons in 2016. In 2016, the standardized prevalence of CD was highest among patients aged 20–29 years, at 10.8 per 100,000. However, the standardized incidence rates were 1.30 per 100,000 for patients aged 10–19 years and 0.88 per 100,000 for those aged 20–29 years. Despite this, there is limited research on patients aged 10–19 years with CD presenting with anal fistula, with most studies involving heterogeneous groups across different age ranges. Therefore, this study aimed to investigate clinical symptoms and surgical findings that could allow early diagnosis of CD in patients with anal fistula aged less 10–19 years.
This study was approved by the Seoul Songdo Hospital Institutional Review Board (approval number 2021-005). Informed consent was waved because of the retrospective study. From January 2009 to December 2020, 320 patients (age <19 years) underwent surgery for anal fistula at the Seoul Songdo Hospital. Among them, we excluded patients who were diagnosed with tuberculosis fistula (n=3) and a patient with missing records (n =1) from the study. Finally, we retrospectively reviewed the medical records of 316 patients (473 fistulas).
Patients with anus-related symptoms who visited the outpatient clinic underwent medical history examination, digital rectal examination, and anoscopy. If necessary, endorectal ultrasonography, three-dimensional pelvic sonography, and magnetic resonance imaging were performed [21, 22]. According to the American Society of Colon and Rectal Surgeons guidelines for anal fistulas, anal fistulas were classified into ‘simple’ and ‘complex’ anal fistulas [6]. Complex anal fistulas include transphincteric fistulas, suprasphincteric, extrasphincteric, and horseshoe fistulas. Simple anal fistulas have none of these complex features and, in general, include intersphincteric and low transphincteric fistulas. Surgery was performed under general or spinal anesthesia; further, outpatient follow-up visits were conducted at 2 and 6 postoperative weeks. Delayed wound healing was defined as incomplete wound healing within 8 postoperative weeks. Diagnosis of CD was determined through comprehensive assessment of symptoms and pathological, endoscopic, and radiological findings [1]. The patients’ age, sex, follow-up duration, past medical history, family history, hematological examination outcomes, and symptoms were analyzed. Family history was defined as a history of IBD in family members. Body weight and body temperature were measured on the same day as the surgery, and the blood test was performed within 1 month before the surgery. Moreover, the characteristics of anal fistula and postoperative wounds as well as colonoscopic and surgical findings were investigated.
All statistical analyses were performed using the IBM SPSS Statistics ver. 22.0 (IBM Corp., Armonk, NY, USA). Continuous data were analyzed using the t-test or Mann-Whitney test. Categorical data were analyzed using the χ2 test and Fisher’s exact test. Statistical significance was set at p<0.05.
Among 316 patients who underwent surgery for anal fistula, 44 patients were diagnosed with CD (CD group), while 272 patients were not diagnosed with CD (non-CD group). Table 1 describes the patient characteristics. The mean age at diagnosis was 16.4 and 17.1 years in the CD and non-CD groups, respectively. Male patients accounted for 93.2% in the CD group, compared to 97.8% in the non-CD group. The mean follow-up duration was 79.8 and 24.5 months in the CD and non-CD groups, respectively. In the CD group, 63.6% and 20.5% had a history of anal abscess and fistula, respectively. The CD group exhibited a significantly higher incidence of patients with a history of anal fistula compared to the non-CD group (p=0.008). In the CD group, 9.1% of patients had a family history of IBD, whereas in the non-CD group, this figure was 0.4%, showing a significant difference between the groups (p=0.001). There was no significant between-group difference in body weight, body temperature, and white blood cell (WBC) count. The level of C-reactive protein (CRP) was 0.7 (0–7) in the CD group and 0 (0–0.6) in the non-CD group, demonstrating a significant difference between the groups (p=0.001).
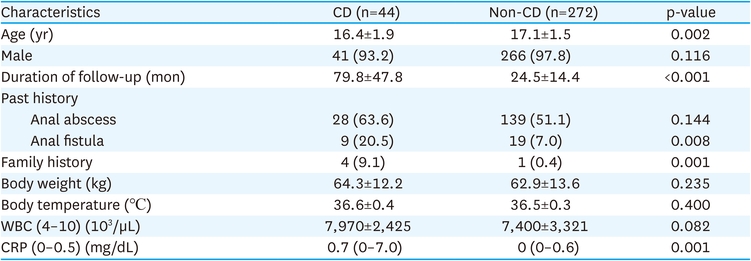
Table 1
Patients demographics
Clinical symptoms were categorized into anal and gastrointestinal symptoms (Table 2). There were no significant between-group differences in anal swelling/prolapse/mass, pain, bleeding, and tenesmus/defecation difficulty. The proportion of patients with anal discharge was 59.1% in the CD group, which was 40.4% in the non-CD group, with a significant between-group difference (p=0.021). The CD group had a significantly higher proportion of patients with weight loss, diarrhea and abdominal pain than the non-CD group (p<0.001). The proportion of patients with complex anal fistula was 43.2% in the CD group, which was significantly higher than that in the non-CD group (p<0.001). There were significant between-group differences in the rate of recurrent and multiple anal fistulas (p=0.023, p=0.001). Factors related to surgical sites were delayed wound healing and friable/edematous/granulation tissue. The proportion of patients with delayed wound healing was significantly higher in the CD group than in the non-CD group (p<0.001). The proportion of patients with friable/edematous/granulation tissue was significantly higher in the CD group than in the non-CD group (p<0.001).
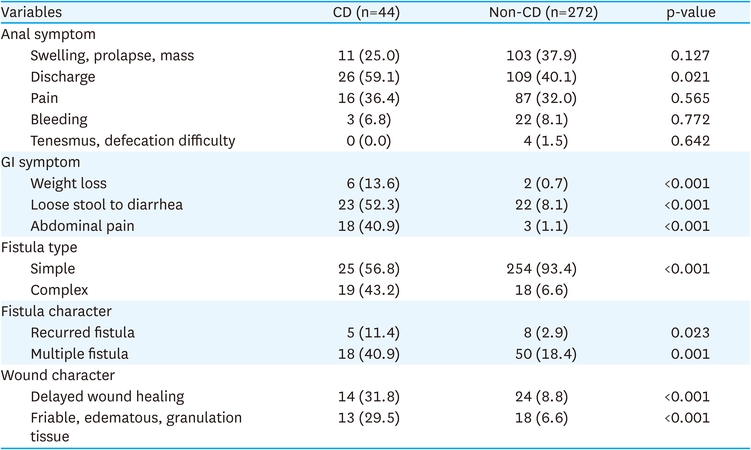
Table 2
Patients symptoms and fistula characters
There were no significant between-group differences in colonoscopy time, time interval between colonoscopy and surgery, hospital day and complications (Table 3). Among the surgical complications, postoperative bleeding usually occurred within 1–7 postoperative days, with some cases recovering after performing procedure to stop bleeding in operating room. Among two patients who developed non-specific complications, one had sore throat and the other one had headache. Simple operations included fistulectomy with lay open, fistulectomy with a stage seton, and fistulectomy with a cutting seton. Complex operations were defined as procedures involving high seton placement with rectal opening or sphincter-saving techniques such as muscle closure. The complex operation was more frequently performed in the CD group (15.9%, p=0.006). Additionally, the number of operations and the number of fistulas were higher in the CD group (p<0.001, p=0.002).
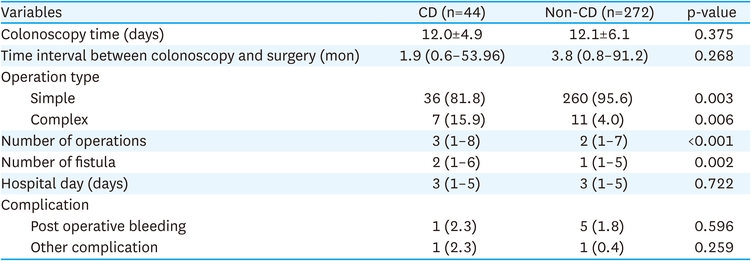
Table 3
Colonoscopy and operation findings
The prevalence of anal fistula is approximately 0.8–2.32 per 10,000 patients [23, 24, 25]; moreover, about 7% of patients who underwent surgery for anal fistula were known to be associated with CD [26]. In our study, among 320 patients aged 10–19 years who underwent surgery for anal fistula, 3 patients were diagnosed before surgery and 41 (12.93%) patients were diagnosed with CD after surgery. The proportion of these patients was higher among individuals aged 10–19 years compared to patients of all age groups. In European countries, 8.2% of children with CD were reported to present anal fistula [7]. Contrastingly, in Korea, 44.8%–50.7% of pediatric patients with CD presented with accompanying anal fistula [27, 28]. Furthermore, CD has been shown to be most common in patients in their 20s. However, the prevalence of CD diagnosed after anal surgery was higher in patients aged 10–19 years than in adult patients. In managing anal fistula cases, it is crucial to initially classify the fistula, trace the ongoing tract, and discuss surgical approaches, as well as potential complications such as anal sphincter injury. However, for patients aged 10–19 years, it is important to first consider whether the anal fistula is associated with CD to guide therapeutic decisions. Performing surgery without considering CD may compromise the doctor-patient relationship due to the occurrence of surgical-related problems, including wound recurrence, delayed wound healing and sphincter damage. For patients present with anal-related symptoms, the risk of CD should be assessed through questioning for symptoms and physical examinations. This is a critical factor influencing symptom improvement, postoperative wound healing, and treatment directions.
Although we observed no significant between-group difference in the sex distribution, most patients in both groups were men. A Korean and foreign study on pediatric patients with CD and anal fistula reported that the proportion of male patients was 43.7%–74.4% [7, 27, 28], and girls were less likely to suffer perianal disease [29]. Our study yielded similar results, further studies are needed to investigate the male predominance in pediatric anal fistula.
A previous study on adult patients with CD and anal fistula reported that the mean time from the diagnosis of anal fistula to CD was 7.6 months (interquartile range, 2.7–26.1 months) [26]. Moreover, abdominal pain, diarrhea, and weight loss were associated with CD diagnosis, while hemorrhoids, anal fissure, anal abscesses, anal surgery, smoking habits, extraintestinal symptoms, or family history of IBD were not. In the present study, the median time from surgery for anal fistula to postoperative colonoscopy was 1.9 months in CD group, 3.8 months in non-CD group, which was relatively shorter than the previously reported values. Consistent with previous studies, we found that a past history of anal fistula, family history of IBD, abdominal pain, diarrhea, weight loss, complex anal fistula, recurrent fistula, and multiple anal fistulas were associated with the diagnosis of CD. However, CD diagnosis was not significantly associated with a history of surgery for anal abscess. Therefore, it is crucial to assess the characteristics of anal fistula as well as symptoms such as abdominal pain, diarrhea, and weight loss in patients aged 10–19 years with anal fistula.
In our study, there was no significant between-group difference in weight, body mass index, WBC count, and fever; however, there was a significant between-group difference in CRP levels. CRP is a crucial protein whose levels increase during acute phase stimulation, including human infection, inflammatory diseases, tissue necrosis, neoplasm, stress, and childbirth [30]. Although there remains controversy, CRP is used as a diagnostic marker for IBD as well as to assess the disease activity, outcomes, and surgery risk of patients with IBD. Our findings suggested that the risk of CD can assessed based on the CRP levels in patients with anal fistulas. The normal CRP level is between 0 and 0.5; notably, the median CRP level in the CD group was 0.7 (minimum 0, maximum 7). Accordingly, it is important to closely monitor patients with increased preoperative CRP levels for symptoms or wound features suggestive of CD.
In our study, there was significant between-group difference in the occurrence of preoperative anal discharge symptoms and complex anal fistula. Anal discharge is a subjectively reported symptom characterized by discharge or sticky substances from the anal opening. An anal fistula is characterized by consistent secretion of internal anal discharge to the external anus through the epithelial lining due to pressure differences or secretion of discharge from anus itself. Anal discharge can result from chronic inflammation and various cytokine-mediated substances.
The postoperative complications of surgery for anal fistula include delayed wound healing and presence of edematous, granulation, or friable tissue. In our study, the rate of delayed wound healing was non-significantly higher in the CD group (31.8%) than in the non-CD group (8.8%). Edematous, granulomatous, and friable tissues do not follow the general process of wound healing. Accordingly, their presence may be indicative of a CD diagnosis even in the absence of CD-suggestive pre- or postoperative findings.
Most studies on CD-related anal fistulas simply considered the presence/absence or recurrence of anal fistulas but did not describe the characteristics of anal fistula itself. Accordingly, our findings are significant as we characterized the morphology of anal fistulas and surgical sites while investigating their relationship with CD, which could provide further insights into anal fistula pathophysiology. Fig. 1 shows the abnormal progression of wound healing at the surgical sites at 76, 101, 139, and 153 days after surgery for anorectal abscess referred from another hospital after incision and drainage. Slight recovery was observed at day 139; however, the wound worsened and did not heal. The patients were diagnosed with CD after colonoscopy. Fig. 2 shows delayed wound healing as well as friable, edematous, and granulation tissues at 57, 55, and 71 postoperative days.
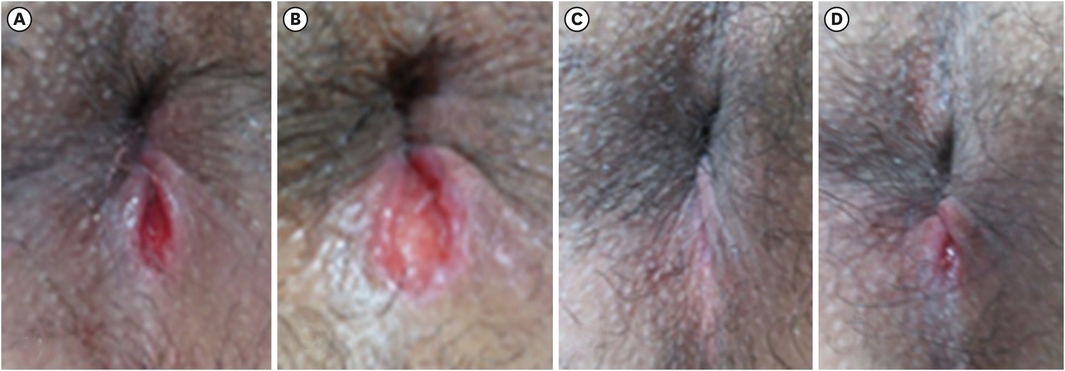
Fig. 1
Delayed wound healing, incision and drain, post operative days: (A) 76 days, (B) 101 days, (C) 139 days, and (D) 153 days.
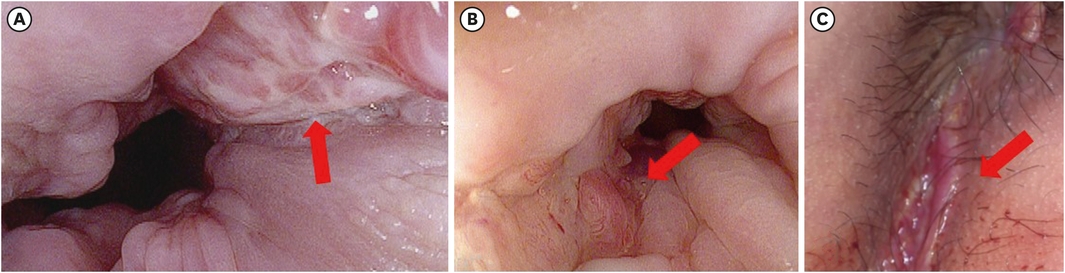
Fig. 2
Delayed wound healing, friable, edematous and granulation tissue, post operative days: (A) 57 days, (B) 55 days, and (C) 71 days.
Colonoscopy is the standard diagnostic method for CD; further, there are current studies on various non-invasive methods, including the fecal calprotectin test and next-generation sequencing. Further caution is required when performing colonoscopy in patients aged 10–19 years since it requires bowel preparation and sedation. In our study, there were no cases of procedure-related complications, including bowel preparation for colonoscopy, sedation, and biopsy, which could be attributed to precautions for bowel preparation and prevent complications. Our findings indicated that patients aged 10–19 years who have anal fistulas with gastrointestinal symptoms can safely undergo colonoscopy, and age should not be the reason for delaying performing a colonoscopy for diagnosis.
Further caution should be applied when performing surgery for anal fistulas since it involves the internal and external anal sphincters, especially who are in growth periods. If CD is diagnosed prior to radical surgeries that damage the sphincters, including modified Hanley operation, fistulectomy, or seton cutting, the surgeries should be conducted after exhausting the treatment options using biological agents and well controlling the intestinal diseases. This approach could minimize complications, including delayed wound healing, gas incontinence, fecal incontinence, or keyhole deformity.
This study has several strengths. First, this study is to investigate the characteristics of CD fistulas in the specific age group of 10–19 years, examining both initial symptom manifestation and outcomes after anal fistula surgery. Second, we performed long-term follow-ups, which allowed extensive review for recurrence of anal fistulas and wound healing.
However, this study has several limitations. First, this was a retrospective study, which has several inherent limitations. Second, the available medical records did not include the frequency and severity of diarrhea as well as the severity and duration of abdominal pain, which were major symptoms. Third, this study may have selection bias since our hospital is specialized for colorectal and anal surgery, and thus may have primarily included patients with high severity. Furthermore, this study only included patients who underwent surgery, despite the fact that in pediatric populations, the spontaneous healing rate of perianal fistulas is often higher than in adults.
In conclusion, for patients aged 10–19 years with anal fistulas presenting symptoms such as anal discharge, elevated CRP levels, complex or recurrent anal fistulas, diarrhea, abdominal pain, and weight loss, emphasizing early suspicion and an active diagnostic work-up is essential for early diagnosis of CD.
PresentationThis study was presented as a poster “Clinical features and colonoscopic findings in patients aged 10–19 years who underwent anal fistula surgery,” at the Korean Society of Coloproctology 55th Annual Meeting, Korea.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.A.Y., L.K.Y., H.K., C.H.
Data curation: K.A.Y., L.K.Y., H.K.
Formal analysis: K.A.Y., C.H.
Investigation: K.A.Y., L.K.Y., H.K., C.H.
Methodology: K.A.Y., L.K.Y.
Project administration: L.K.Y., C.H.
Validation: K.A.Y., L.K.Y.
Visualization: K.A.Y., H.K.
Writing - original draft: K.A.Y., L.K.Y., H.K., C.H.
Writing - review & editing: K.A.Y., L.K.Y., H.K., C.H.
