ABSTRACT
-
Purpose
This study investigated the clinical characteristics, anatomical distribution, operative management, and postoperative outcomes of pediatric patients who underwent surgery for intestinal duplication and were registered through a nationwide multicenter survey conducted by the Korean Association of Pediatric Surgeons (KAPS).
-
Methods
KAPS conducted a nationwide multicenter retrospective survey across 18 institutions between 2020 and 2024 and collected data from 144 patients.
-
Results
Female patients accounted for 55.6% of surgically treated cases, corresponding to a male to female ratio of 1:1.25. Vomiting and abdominal pain were the most common presenting symptoms. Prenatal diagnosis was achieved in 43.7% of cases. The ileum was the most common site of intestinal duplication (41.0%). Cystic duplications predominated (82.6%), and communication with the native bowel was documented in 19.4% of cases. Elective surgery was performed in 83.3% of patients, with laparoscopic-assisted surgery being the most commonly used approach (52.8%). The most frequently performed surgical procedures were excision (49.3%) and bowel resection with anastomosis (47.2%). Recurrence occurred in three patients (2.1%), and mortality was reported in one patient (0.7%).
-
Conclusion
This study represents the largest multicenter dataset on intestinal duplication in South Korea and provides comprehensive information regarding its clinical characteristics and surgical outcomes. These findings may serve as a useful reference for understanding the clinical spectrum and operative management of pediatric intestinal duplication in South Korea and may support the development of future standardized prospective studies.
-
Keywords: Intestinal duplication; Child; Surveys and questionnaires; Laparoscopy
INTRODUCTION
Intestinal duplications are rare congenital anomalies that can occur anywhere along the alimentary tract, most commonly in the small intestine [
1-
3]. They occur in approximately 1 in 4,500 live births and are most frequently diagnosed in neonates and children [
4-
6]. The clinical presentation of intestinal duplication varies according to morphological type, anatomical location, and patient age group. Presentations range from incidental prenatal detection to dysphagia, abdominal pain, abdominal mass, intussusception, inflammation, bleeding, and even peritonitis secondary to perforation. Because of the rarity of this condition and its nonspecific clinical manifestations, achieving an accurate preoperative diagnosis is often challenging. Definitive treatment generally requires complete surgical excision, as residual lesions after partial excision may predispose patients to recurrence, and even clinically silent duplications may subsequently result in complications [
6]. Despite numerous single-center reports, nationwide multicenter data regarding surgically treated pediatric cases remain limited. Therefore, we report the findings of a nationwide multicenter Korean survey coordinated by the Korean Association of Pediatric Surgeons (KAPS), detailing demographic characteristics, prenatal diagnosis, clinical manifestations, associated anomalies, preoperative diagnostic methods, anatomical location and type of intestinal duplication, presence of communication and ectopic tissue, operative management, and postoperative outcomes in patients with intestinal duplication, with particular emphasis on how lesion characteristics inform surgical decision-making.
METHODS
We retrospectively reviewed the medical records of pediatric patients who underwent surgery for intestinal duplication at 18 KAPS institutions between January 2020 and December 2024. The KAPS committee developed a case registration form to collect data regarding patient sex, birth weight, gestational age, prenatal diagnosis, clinical manifestations, associated anomalies, preoperative diagnostic methods, anatomical location and type of intestinal duplication, presence of communication and ectopic tissue, operative management, and postoperative outcomes. The form was distributed by email to 18 pediatric surgical centers and completed by authorized KAPS members at the participating centers, yielding data from 144 patients. Patients were eligible if they were <18 years of age and underwent surgical treatment for intestinal duplication during the specified 5-year study period. Cases with insufficient data were excluded. Because the survey included cases reported by 18 participating KAPS-affiliated pediatric surgical centers, the dataset represents a multicenter surgical registry rather than a population-based national incidence database.
Ethics statement
The study protocol was approved by the Institutional Review Board of Kyungpook National University Hospital (No. 2025-06-005). Informed consent was waived due to the use of deidentified data and the retrospective nature of the study.
RESULTS
Registered case numbers
A total of 144 patients with intestinal duplication were registered in this nationwide survey. The annual case distribution was as follows: 39 cases in 2020, 28 in 2021, 25 in 2022, 27 in 2023, and 25 in 2024. The regional distribution was as follows: 114 cases (79.1%) from the Seoul/Gyeonggi region, 16 cases (11.1%) from the Busan/Ulsan/Gyeongnam region, six cases (4.2%) from Daegu, six cases (4.2%) from the Jeolla region, and two cases (1.4%) from the Chungcheong region. This distribution suggests a concentration of registered cases in the Seoul/Gyeonggi region, likely reflecting referral patterns and the geographic distribution of participating tertiary centers.
Patient demographics and perinatal characteristics
The cohort included 64 male patients (44.4%) and 80 female patients (55.6%), yielding a male to female ratio of approximately 1:1.25 and demonstrating a predominance of female patients in this surgical series. A total of 115 patients (79.9%) were born at a gestational age of ≥37 weeks, and 113 patients (78.5%) had a birth weight of ≥2,500 g. The median age at surgery was 8.5 months (range, 1 day–17 years). Prenatal diagnosis was confirmed in 63 patients (43.7%). Among the subset of patients for whom this information was available, the mean gestational age at prenatal diagnosis was 25.6 weeks. Maternal polyhydramnios was absent in 105 patients (72.9%). No family history of intestinal duplication was reported among any of the 144 patients (
Table 1).
Clinical manifestations at diagnosis included vomiting in 39 patients (27.1%), making it the most common presenting symptom, followed by abdominal pain in 35 patients (24.3%) and abdominal mass in 16 patients (11.1%). Abdominal distention was observed in 11 patients (7.6%), hematochezia in 10 patients (6.9%), abnormal anal appearance or discharge in eight patients (5.6%), and fever in seven patients (4.9%). However, 80 patients (55.6%) were asymptomatic at the time of diagnosis (
Table 2).
Cardiovascular anomalies were the most frequently observed associated anomalies, occurring in 10 patients, followed by craniofacial and musculoskeletal anomalies in seven patients. Other associated anomalies included gastrointestinal anomalies in four patients, central nervous system anomalies in four, genitourinary anomalies in four, and chromosomal abnormalities in three.
Preoperative diagnostic methods
Multiple diagnostic modalities were used in some patients. The most frequently performed preoperative imaging studies were abdominal radiography in 122 patients (84.7%) and abdominal ultrasonography in 120 patients (83.3%). Other diagnostic modalities included abdominal computed tomography (CT) in 57 patients (39.6%), abdominal magnetic resonance imaging (MRI) in 21 (14.6%), upper gastrointestinal series or small bowel series in 13 (9.0%), colon studies in 13 (9.0%), Meckel scans in seven (4.9%), colonoscopy in five (3.5%), and endoscopy in three (2.1%). These findings indicate that conventional radiography and ultrasonography were strongly preferred for initial evaluation in clinical practice.
Location and type of intestinal duplication
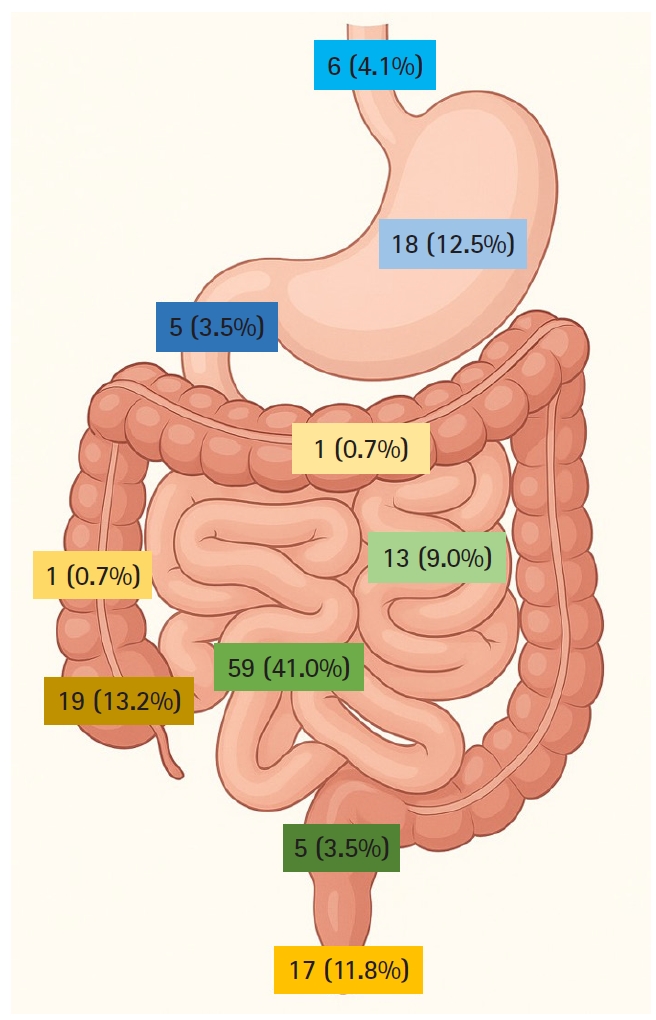
The ileum was the most common site of intestinal duplication, occurring in 59 cases (41.0%). Other locations included the cecum in 19 cases (13.2%), stomach in 18 cases (12.5%), anus in 17 cases (11.8%), jejunum in 13 cases (9.0%), esophagus in six cases (4.1%), duodenum in five cases (3.5%), rectum in five cases (3.5%), and colon in two cases (1.4%) (
Fig. 1). Multiple duplications were identified in two patients: one patient had two duplications in the ileum, and one had duplications in both the jejunum and ileum. For anatomical classification, the patient with two ileal duplications was counted as one ileal case, and the patient with one jejunal and one ileal duplication was also counted as one ileal case. Most intestinal duplications were cystic, accounting for 119 cases (82.6%), whereas tubular duplications were identified in 20 cases (13.9%). In five cases (3.5%), the type was unknown. This distribution indicates that cystic duplications predominated across nearly all locations except the anus, where tubular duplications were more frequent (
Table 3).
Communication between the duplication and the adjacent native intestinal lumen was identified in 28 patients (19.4%), whereas 107 patients (74.3%) had no communication. Communication status was unknown in nine cases (6.3%).
Table 4 summarizes communication between the intestinal duplication and the adjacent bowel according to anatomical location. These findings indicate that most intestinal duplications did not communicate with the native intestinal tract, although communication was relatively more frequent in duodenal and rectal duplications.
Ectopic tissue was identified in 21 of 144 patients (14.6%), whereas 123 patients (85.4%) had no ectopic tissue.
Table 4 also shows the distribution of ectopic tissue in intestinal duplications according to anatomical location. These findings suggest that ectopic gastric or pancreatic tissue was most frequently identified in duplications located in the ileum and duodenum.
Among the patients, 112 had data allowing comparison of intestinal duplication size between initial diagnosis and surgery. Of these, 67 cases (59.8%) increased in size, 31 (27.7%) decreased in size, and 14 (12.5%) showed no change.
Operative treatment of intestinal duplication
Among the 144 patients with intestinal duplication, elective surgery was performed in 120 (83.3%), whereas emergency surgery was required in 24 (16.7%). A breakdown by anatomical location is shown in
Table 5. These findings indicate that most patients underwent planned elective surgery, although emergency intervention was more frequently required for duplications located in the jejunum, ileum, and cecum than for those in other locations.
The most commonly used surgical approach was laparoscopic-assisted surgery, performed in 76 patients (52.8%), followed by open surgery in 40 patients (27.8%), pure laparoscopic surgery in 26 patients (18.0%), and thoracoscopic surgery in two patients (1.4%).
Table 6 summarizes operative modalities for intestinal duplication according to anatomical location. These findings highlight the increasing preference for minimally invasive techniques, particularly laparoscopic-assisted surgery, in the treatment of intestinal duplication, especially in the small intestine. However, open surgery remained predominant for anorectal or anal lesions.
The most commonly used operative methods were excision in 71 cases (49.3%) and bowel resection with anastomosis in 68 cases (47.2%). Less common procedures included partial excision in two cases (1.4%) and other methods in three cases (2.1%). A breakdown by anatomical location is shown in
Table 7. These findings suggest that excision and bowel resection with anastomosis were the two main surgical strategies and were selected according to lesion location, communication with the native bowel, and involvement of surrounding structures.
Postoperative complications occurred in both the early and late postoperative periods. Early complications occurred in six patients and included wound infection in five cases (duodenal duplication, one; jejunal duplication, one; ileal duplication, three) and anastomotic leakage in one case involving duodenal duplication. A late postoperative complication was observed in one patient with duodenal duplication, who developed intestinal obstruction. Recurrence was observed in three of 144 patients (2.1%): one with esophageal duplication, one with duodenal duplication, and one with rectal duplication. One notable case involved a female patient who underwent reoperation for remnant rectal duplication cysts over several years after initial involvement of both the colon and rectum. One death occurred (0.7%), involving a patient with duodenal duplication. The cause of death was pulmonary hypertension during the healing phase after anastomotic leakage.
DISCUSSION
Intestinal duplication is a rare congenital anomaly characterized by a well-formed cystic or tubular structure that is attached to, or shares a common wall with, the alimentary tract; is lined by gastrointestinal mucosa; and has a well-developed smooth muscle layer [
3,
4,
7].
The exact pathogenetic mechanism underlying intestinal duplication remains unclear. Several mechanisms have been proposed, including the split notochord theory, abnormal recanalization of the transiently solid gastrointestinal tract during embryogenesis, abortive twinning, persistence of embryological diverticula, and intrauterine vascular accidents. These hypotheses reflect the complex, multifactorial nature of this congenital anomaly [
8].
Although intestinal duplication has traditionally been reported more frequently in male patients, Sujka et al. [
9] observed a female predominance, with 62.0% of cases occurring in female patients. Similarly, intestinal duplication was more common in female patients in our series, accounting for 55.6% of cases.
The clinical manifestations of intestinal duplication vary widely depending on patient age, anatomical location, duplication cyst size, and presence of ectopic mucosa [
4]. In our nationwide survey, vomiting (27.1%) and abdominal pain (24.3%) were the most common symptoms, whereas a substantial proportion of patients (55.6%) were incidentally diagnosed without symptoms. These findings are consistent with those of previous studies [
4,
10].
In our nationwide survey, the ileum was the most common location of intestinal duplication (41.0%), followed by the cecum (13.2%), stomach (12.5%), anus (11.8%), and jejunum (9.0%). This distribution was comparable to that reported in previous studies [
1,
3]. In our series, 82.6% of intestinal duplications were cystic, consistent with previous reports [
4,
9].
Most cases in our cohort (74.3%) showed no communication with the adjacent bowel, consistent with previously published data [
4]. However, intestinal duplications involving the duodenum and rectum demonstrated relatively high rates of communication with the native bowel (60.0% in each location), which may substantially influence surgical decision-making and treatment strategy.
Compared with the study by Guerin et al. [
7], which reported ectopic tissue in 41.0% of cases, our series demonstrated a lower prevalence of ectopic tissue (14.6%). Complete mucosal excision is particularly important in intestinal duplications with ectopic tissue, as retained mucosa may contribute to complications such as bleeding, ulceration, and recurrence.
With the increasing use of prenatal ultrasonography, the number of intestinal duplications diagnosed before birth has steadily increased. In our nationwide survey, 43.7% of patients were diagnosed at a mean gestational age of 25.6 weeks among those with available data, comparable to rates reported in previous studies [
2,
5]. This relatively high prenatal detection rate underscores the value of prenatal ultrasonography for prompting postnatal surveillance and timely consultation.
In our nationwide survey, plain abdominal radiography and ultrasonography were the most widely used preoperative studies, reflecting their accessibility and diagnostic utility. Abdominal ultrasonography typically reveals a cystic lesion adjacent to the intestine with a characteristic double-wall or muscular rim sign, reflecting an inner hyperechoic mucosal layer and an outer hypoechoic smooth muscle layer [
1]. Cross-sectional imaging, including CT and MRI, as well as contrast studies, can assess lesion location, vascularity, and communication, thereby facilitating surgical planning. On abdominal CT, intestinal duplication usually appears as a well-defined, low-attenuation, unilocular cystic mass that is most commonly round or spherical and often lacks apparent communication with the native bowel. In some cases, however, the duplication may appear as a tubular structure continuous with the intestinal lumen.
Complete surgical excision remains the mainstay of treatment for intestinal duplication [
11-
13]. Partial excision is associated with an increased risk of recurrence, and even asymptomatic lesions may lead to future complications [
14]. In this survey, all three cases of recurrence were observed following cyst excision. These recurrences occurred not only after partial excision but also after complete excision, indicating that meticulous follow-up is warranted regardless of the extent of excision. According to Ma et al. [
15], malignant transformation in intestinal duplication is rare but carries an unfavorable prognosis, supporting the need for definitive surgical treatment. Therefore, careful selection of the surgical strategy is essential, and the optimal approach should be determined according to the size and location of the cyst and its anatomical relationship with the adjacent intestine. The most commonly used surgical techniques in our series were simple excision (49.3%) and bowel resection with anastomosis (47.2%). Bowel resection with anastomosis was used more frequently for jejunoileal and cecal lesions, in which shared walls or vascularity often preclude safe enucleation. Conversely, simple excision or enucleation is particularly favored in locations where bowel resection with anastomosis should be avoided, such as the esophagus, stomach, and duodenum [
16]. Selective mucosal excision has been described as an effective treatment strategy in rare cases of extensive tubular intestinal duplication [
1]. Recently, minimally invasive laparoscopic surgery has been increasingly adopted for intestinal duplication [
9,
11,
14,
16]. In our series, laparoscopic and laparoscopic-assisted procedures were frequently used, particularly for small intestinal lesions; however, because complications were not analyzed according to operative approach, comparative safety cannot be inferred. With advances in imaging modalities, an increasing number of intestinal duplications are being detected during prenatal evaluation, leading to ongoing debate regarding the optimal timing of surgical intervention [
17-
20]. Laje et al. [
18] suggested that early surgical treatment after birth is warranted because intestinal duplication can cause substantial complications. In a systematic review by Fahy and Pierro [
19], almost half of prenatally diagnosed patients developed symptoms early in life and required surgical intervention, whereas close observation with delayed prophylactic resection during infancy was recommended for asymptomatic patients. Similarly, Wang et al. [
20] reported that intestinal obstruction is the most common complication of intestinal duplication and occurs predominantly during the neonatal period. They concluded that symptomatic patients require early intervention, whereas asymptomatic patients can be managed with close observation and delayed resection. Early surgical resection can be considered for duplications with a diameter greater than 3 cm or those of the intraluminal type. Therefore, the timing of surgery should be individualized according to the size and location of the duplication cyst and its potential for complications.
This nationwide multicenter survey of 144 children treated for intestinal duplication across 18 KAPS institutions represents the largest Korean dataset to date and provides several practice-relevant insights. Nevertheless, this study has important limitations. Its retrospective design may have introduced selection and information bias. Substantial heterogeneity in anatomical location, clinical presentation, and disease extent, combined with the multicenter nature of the data, likely influenced surgical decision-making and perioperative management. Variations in institutional experience and operative preferences limit direct comparisons among surgical approaches and reflect differences in local practice patterns across institutions. However, these nationwide data provide an important foundation for identifying consensus-based strategies and may facilitate the future development of a standardized KAPS clinical pathway for the management of intestinal duplication. Future research should focus on prospective multicenter studies with standardized data collection and treatment protocols. Stratification according to anatomical location and clinical characteristics will help define optimal surgical strategies and long-term outcomes in patients with intestinal duplication.
NOTES
-
Authors’ contributions
Conceptualization: DK, HK, DYK, SCK, SHK, WK, HYK, SHN, JMN, SP, JBP, MJB, JMS, JYS, JS, SMA, HBY, JTO, CO, JKY, SL, JYL, CL, KI, SMJ, YJJ, EJ, JHC, MJC, SH, SJH, IGH, JYP. Data curation: JYP. Investigation: all authors. Methodology: DK, HK, DYK, SCK, SHK, WK, HYK, SHN, JMN, SP, JBP, MJB, JMS, JYS, JS, SMA, HBY, JTO, CO, JKY, SL, JYL, CL, KI, SMJ, YJJ, EJ, JHC, MJC, SH, SJH, IGH, JYP. Resources: DK, HK, DYK, SCK, SHK, WK, HYK, SHN, JMN, SP, JBP, MJB, JMS, JYS, JS, SMA, HBY, JTO, CO, JKY, SL, JYL, CL, KI, SMJ, YJJ, EJ, JHC, MJC, SH, SJH, IGH. Visualization: JYP. Writing–original draft: JYP. Writing–review & editing: all authors. All authors read and approved the final manuscript.
-
Conflict of interest
Jinyoung Park, Soo-Hong Kim, So Hyun Nam, Jung-Man Namgoong, Junbeom Park, Ji-Young Sul, Hee-Beom Yang, Sanghoon Lee, Ju Yeon Lee, Kyong Ihn, Yeon Jun Jeong, Jae Hee Chung, and Min Jeng Cho are editorial board members of this journal, but were not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
All data generated or analyzed during this study are included in this published article. For other data, these may be requested through the corresponding author.
Fig. 1.Distribution of intestinal duplication according to anatomical location.
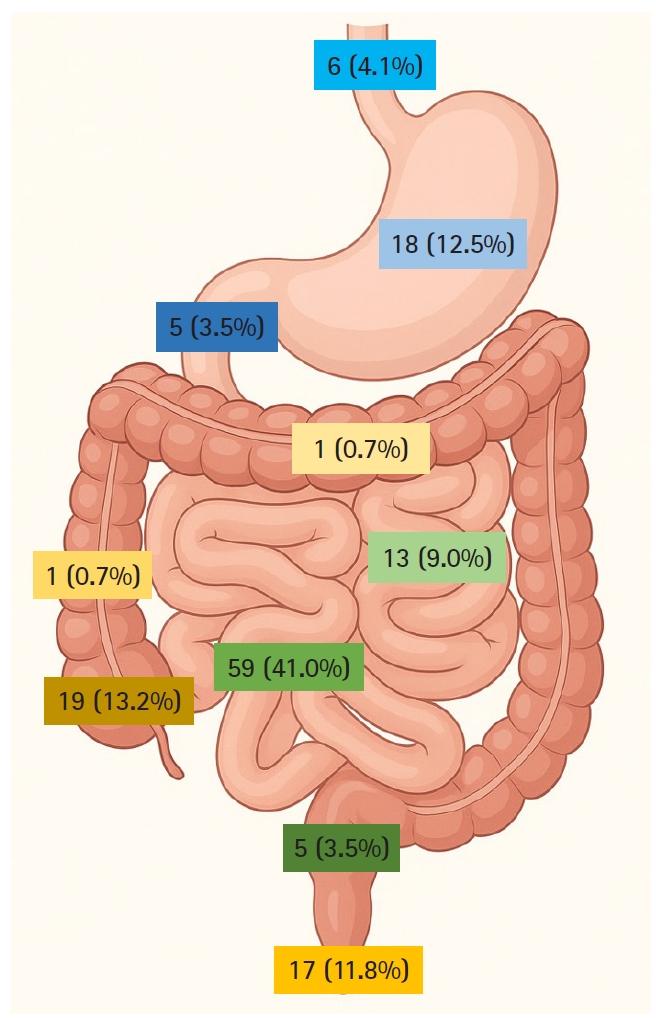
Table 1.Patient demographics and perinatal characteristics
Table 1.
|
Characteristic |
No. (%) |
|
Sex |
|
|
Male |
64 (44.4) |
|
Female |
80 (55.6) |
|
Gestational age (wk) |
|
|
<37 |
15 (10.4) |
|
≥37 |
115 (79.9) |
|
Not available |
14 (9.7) |
|
Birth weight (g) |
|
|
<2,500 |
12 (8.3) |
|
≥2,500 |
113 (78.5) |
|
Not available |
19 (13.2) |
|
Prenatal diagnosis |
|
|
Yes |
63 (43.7) |
|
No |
76 (52.8) |
|
Not available |
5 (3.5) |
|
Polyhydramnios |
|
|
Yes |
1 (0.7) |
|
No |
105 (72.9) |
|
Not available |
38 (26.4) |
Table 2.
Table 2.
|
Clinical manifestation |
No. (%) |
|
Absence of symptoms |
80 (55.6) |
|
Vomiting |
39 (27.1) |
|
Abdominal pain |
35 (24.3) |
|
Abdominal mass |
16 (11.1) |
|
Abdominal distension |
11 (7.6) |
|
Hematochezia |
10 (6.9) |
|
Abnormal anal appearance or discharge |
8 (5.6) |
|
Fever |
7 (4.9) |
|
Melena |
4 (2.8) |
|
Constipation |
2 (1.4) |
|
Dysphagia |
2 (1.4) |
Table 3.Location and type of intestinal duplication
Table 3.
|
Location |
Cystic type |
Tubular type |
Unknown type |
|
Esophagus |
6 (100) |
0 (0) |
0 (0) |
|
Stomach |
18 (100) |
0 (0) |
0 (0) |
|
Duodenum |
4 (80.0) |
1 (20.0) |
0 (0) |
|
Jejunum |
10 (76.9) |
3 (23.1) |
0 (0) |
|
Ileum |
57 (96.6) |
1 (1.7) |
1 (1.7) |
|
Cecum |
17 (89.5) |
0 (0) |
2 (10.5) |
|
Colon |
1 (50.0) |
1 (50.0) |
0 (0) |
|
Rectum |
4 (80.0) |
1 (20.0) |
0 (0) |
|
Anus |
2 (11.8) |
13 (76.4) |
2 (11.8) |
|
Total |
119 (82.6) |
20 (13.9) |
5 (3.5) |
Table 4.Presence of communication with native bowel and ectopic tissue according to anatomical location
Table 4.
|
Location |
Communication
|
Ectopic tissue
|
|
+ |
− |
Unknown |
+ |
− |
|
Esophagus |
1 (16.7) |
5 (83.3) |
0 (0) |
0 (0) |
6 (100) |
|
Stomach |
4 (22.2) |
14 (77.8) |
0 (0) |
1 (5.6)a)
|
17 (94.4) |
|
Duodenum |
3 (60.0) |
2 (40.0) |
0 (0) |
2 (40.0)b)
|
3 (60.0) |
|
Jejunum |
1 (7.7) |
10 (76.9) |
2 (15.4) |
2 (15.4)c)
|
11 (84.6) |
|
Ileum |
8 (13.6) |
46 (77.9) |
5 (8.5) |
14 (23.7)d)
|
45 (76.3) |
|
Cecum |
7 (36.8) |
11 (57.9) |
1 (5.3) |
2 (10.5)e)
|
17 (89.5) |
|
Colon |
1 (50.0) |
1 (50.0) |
0 (0) |
0 (0) |
2 (100) |
|
Rectum |
3 (60.0) |
1 (20.0) |
1 (20.0) |
0 (0) |
5 (100) |
|
Anus |
0 (0) |
17 (100) |
0 (0) |
0 (0) |
17 (100) |
|
Total |
28 (19.4) |
107 (74.3) |
9 (6.3) |
21 (14.6) |
123 (85.4) |
Table 5.Elective versus emergency surgery according to location
Table 5.
|
Location |
Elective |
Emergency |
|
Esophagus |
6 (100) |
0 (0) |
|
Stomach |
17 (94.4) |
1 (5.6) |
|
Duodenum |
5 (100) |
0 (0) |
|
Jejunum |
9 (69.2) |
4 (30.8) |
|
Ileum |
47 (79.7) |
12 (20.3) |
|
Cecum |
12 (63.2) |
7 (36.8) |
|
Colon |
2 (100) |
0 (0) |
|
Rectum |
5 (100) |
0 (0) |
|
Anus |
17 (100) |
0 (0) |
|
Total |
120 (83.3) |
24 (16.7) |
Table 6.
Table 6.
|
Location |
Thoracoscopy |
Laparoscopy |
Laparoscopic-assisted |
Open |
|
Esophagus |
2 (33.3) |
4 (66.7) |
0 (0) |
0 (0) |
|
Stomach |
0 (0) |
16 (88.8) |
1 (5.6) |
1 (5.6) |
|
Duodenum |
0 (0) |
2 (40.0) |
1 (20.0) |
2 (40.0) |
|
Jejunum |
0 (0) |
0 (0) |
10 (76.9) |
3 (23.1) |
|
Ileum |
0 (0) |
0 (0) |
50 (84.7) |
9 (15.3) |
|
Cecum |
0 (0) |
1 (5.3) |
12 (63.1) |
6 (31.6) |
|
Colon |
0 (0) |
1 (50.0) |
1 (50.0) |
0 (0) |
|
Rectum |
0 (0) |
2 (40.0) |
1 (20.0) |
2 (40.0) |
|
Anus |
0 (0) |
0 (0) |
0 (0) |
17 (100) |
|
Total |
2 (1.4) |
26 (18.0) |
76 (52.8) |
40 (27.8) |
Table 7.Operative methods according to location
Table 7.
|
Location |
BRA |
Excision |
Partial excision |
Others |
|
Esophagus |
0 (0) |
5 (83.3) |
0 (0) |
1 (16.7) |
|
Stomach |
3 (16.7) |
14 (77.8) |
1 (5.5) |
0 (0) |
|
Duodenum |
1 (20.0) |
4 (80.0) |
0 (0) |
0 (0) |
|
Jejunum |
10 (76.9) |
3 (23.1) |
0 (0) |
0 (0) |
|
Ileum |
38 (64.4) |
20 (33.9) |
1 (1.7) |
0 (0) |
|
Cecum |
14 (73.7) |
4 (21.0) |
0 (0) |
1 (5.3) |
|
Colon |
2 (100) |
0 (0) |
0 (0) |
0 (0) |
|
Rectum |
0 (0) |
5 (100) |
0 (0) |
0 (0) |
|
Anus |
0 (0) |
16 (94.1) |
0 (0) |
1 (5.9) |
|
Total |
68 (47.2) |
71 (49.3) |
2 (1.4) |
3 (2.1) |
REFERENCES
- 1. Xiang L, Lan J, Chen B, Li P, Guo C. Clinical characteristics of gastrointestinal tract duplications in children: a single-institution series review. Medicine (Baltimore) 2019;98:e17682.
- 2. Wang M, Wang L, Chen Y, Qian Y, Chen Q. Clinical characteristics and treatment of gastric duplications in children. J Pediatr Surg 2025;60:162115.
- 3. Sanguesa Nebot C, Llorens Salvador R, Carazo Palacios E, Pico Aliaga S, Ibanez Pradas V. Enteric duplication cysts in children: varied presentations, varied imaging findings. Insights Imaging 2018;9:1097-106.
- 4. Kim SH, Cho YH, Kim HY. Alimentary tract duplication in pediatric patients: Its distinct clinical features and managements. Pediatr Gastroenterol Hepatol Nutr 2020;23:423-9.
- 5. Destro F, Marinaro M, Durante E, et al. A retrospective analysis of alimentary tract duplications in pediatric patients: a 14-year single-center experience. Pediatr Surg Int 2024;40:283.
- 6. Dreznik Y, Almog A, Paran M, Konen O, Kravarusic D. Small bowel duplication cyst in the pediatric population: when to operate? Pediatr Surg Int 2025;41:56.
- 7. Guerin F, Podevin G, Petit T, et al. Outcome of alimentary tract duplications operated on by minimally invasive surgery: a retrospective multicenter study by the GECI (Groupe d'Etude en Coeliochirurgie Infantile). Surg Endosc 2012;26:2848-55.
- 8. Losefsky Q. A comprehensive review of enteric duplication cysts, their pathophysiology, presentation, and treatment. J Clin Exp Gastroenterol 2022;1:1-4.
- 9. Sujka JA, Sobrino J, Benedict LA, Alemayehu H, Peter SS, Hendrickson R. Enteric duplication in children. Pediatr Surg Int 2018;34:1329-32.
- 10. Yan J, Lei W, Yan J, Ding C, Liu T, Chen Y. Ileocecal duplication in children: a single-center experience of 115 cases. Eur J Pediatr 2022;181:3937-44.
- 11. Shchapov N, Kulikov D, Ekimovskaya E, Sergeyeva S, Andreyeva E, Ivanitskaya O. Laparoscopic cyst enucleation is a promising technique for treatment of gastrointestinal tract duplications in children. J Pediatr Surg 2023;58:658-63.
- 12. Yan J, Yan J, Ding C, Guo J, Peng Y, Chen Y. Clinical features of colorectal duplication in children: a study of 25 cases. J Pediatr Surg 2022;57:97-101.
- 13. Laplanche U, Montalva L, Dara P, et al. Enucleation for intestinal duplications: a comparative study with intestinal resection and anastomosis. Pediatr Surg Int 2024;40:167.
- 14. Patino Mayer J, Bettolli M. Alimentary tract duplications in newborns and children: diagnostic aspects and the role of laparoscopic treatment. World J Gastroenterol 2014;20:14263-71.
- 15. Ma H, Xiao W, Li J, Li Y. Clinical and pathological analysis of malignancies arising from alimentary tract duplications. Surg Oncol 2012;21:324-30.
- 16. Gorecki W, Bogusz B, Zajac A, Soltysiak P. Laparoscopic and laparoscopy-assisted resection of enteric duplication cysts in children. J Laparoendosc Adv Surg Tech A 2015;25:838-40.
- 17. Foley PT, Sithasanan N, McEwing R, Lipsett J, Ford WD, Furness M. Enteric duplications presenting as antenatally detected abdominal cysts: is delayed resection appropriate? J Pediatr Surg 2003;38:1810-3.
- 18. Laje P, Flake AW, Adzick NS. Prenatal diagnosis and postnatal resection of intraabdominal enteric duplications. J Pediatr Surg 2010;45:1554-8.
- 19. Fahy AS, Pierro A. A systematic review of prenatally diagnosed intra-abdominal enteric duplication cysts. Eur J Pediatr Surg 2019;29:68-74.
- 20. Wang L, Zhang S, Wang M, et al. Postnatal clinical features and surgical strategies of gastrointestinal tract duplications diagnosed prenatally. J Pediatr Surg 2025;60:162325.

 , Dayoung Ko2
, Dayoung Ko2