ABSTRACT
-
Purpose
This study aimed to compare perioperative outcomes between laparoscopic-assisted diverticulectomy and laparoscopic-assisted small bowel resection for Meckel diverticulum.
-
Methods
This single-center retrospective comparative cohort study included 39 patients who underwent laparoscopic-assisted surgery for Meckel diverticulum at Samsung Medical Center, Korea, between June 2010 and December 2023. Patients were classified into the laparoscopic-assisted diverticulectomy group or the laparoscopic-assisted small bowel resection group. Baseline characteristics, preoperative presentation, operative time, time to first oral feeding, postoperative hospital stay, complications, reoperation, and follow-up outcomes were compared between groups.
-
Results
Of the 39 patients, 19 underwent laparoscopic-assisted diverticulectomy and 20 underwent laparoscopic-assisted small bowel resection. Baseline characteristics and preoperative presentation did not differ significantly between groups. Operative time was significantly shorter in the diverticulectomy group than in the small bowel resection group (median, 55.0 vs. 76.0 minutes; P=0.002). Time to first oral feeding did not differ significantly between groups (median, 2 days [2–2 days] vs. 2 days [1–3 days]; P=0.397). Postoperative hospital stays also did not differ significantly between groups (median, 4 days [3–4 days] vs. 4 days [4–5 days]; P=0.118), although hospitalization tended to be longer in the laparoscopic-assisted small bowel resection group. No statistically significant difference in complication rates was observed between groups; however, the number of events was low, limiting definitive comparison.
-
Conclusion
Laparoscopic-assisted diverticulectomy was associated with shorter operative time and a tendency toward shorter postoperative hospital stay than small bowel resection, without an observed increase in early complications. It may be a reasonable option for carefully selected patients with uncomplicated Meckel diverticulum.
-
Keywords: Cohort studies; Meckel diverticulum; Laparoscopy; Length of stay; Operative time
INTRODUCTION
Background
Meckel diverticulum arises from incomplete closure of the omphalomesenteric duct during early development. It is among the most common congenital intestinal anomalies, affecting 0.3% to 2.7% of the population [
1,
2]. The duct provides nutrition until placental formation and normally separates from the intestine by the seventh week of gestation. Failure of complete separation may result in cysts, fistulas, or fibrous bands that can cause obstruction. In the absence of additional attachments, Meckel diverticulum may form. Classically, Meckel diverticulum has been described by the “rule of twos”: it affects approximately 2% of the population, measures approximately 5 cm (2 inches) in length, is located approximately 60 cm (2 feet) from the ileocecal valve in the ileum, is twice as common in males, and may contain two types of ectopic tissue, gastric or pancreatic. Ectopic gastric or pancreatic tissue can secrete acid and pepsin, leading to ulceration of the adjacent ileal mucosa and gastrointestinal bleeding. This bleeding is usually painless and may be brisk or massive, causing stool to appear bright red, brick red, or black. Intestinal obstruction is another common complication. It can occur through several mechanisms, including volvulus around a fibrous band, intussusception, Littre hernia, entrapment of the small bowel beneath the diverticular blood supply, stricture from chronic diverticulitis, or Meckel diverticulum lithiasis [
3]. Surgeons treat Meckel diverticulum with either diverticulectomy or small bowel resection with anastomosis, depending on the diverticulum anatomy, base width, complications such as ischemia or perforation, and the presence of ectopic gastric tissue [
3,
4].
Traditionally, symptomatic Meckel diverticulum has been managed with excision through laparotomy, using either segmental small bowel resection or wedge resection with anastomosis. Minimally invasive techniques now enable laparoscopic-assisted excision, and the use of laparoscopic stapling devices for intracorporeal diverticulectomy is increasingly common [
5]. The choice between diverticulectomy and small bowel resection is particularly relevant for diverticula with a wide base or those complicated by bleeding or inflammation, because ectopic tissue can extend into the adjacent ileum [
6]. However, direct comparisons of perioperative outcomes between laparoscopic-assisted diverticulectomy (LA-D) and laparoscopic-assisted small bowel resection (LA-SBR) remain limited.
Therefore, this study aimed to evaluate perioperative characteristics and postoperative outcomes according to the type of laparoscopic-assisted procedure performed for Meckel diverticulum.
METHODS
Ethics statement
This retrospective study was approved by the Institutional Review Board at Samsung Medical Center (No. 2026-01-058). Informed consent was waived due to the use of deidentified data and the retrospective nature of the study.
Study design
This was a single-center retrospective comparative cohort study. We included 39 patients with Meckel diverticulum who underwent surgery at Samsung Medical Center from June 2010 to December 2023.
Surgical procedures
The surgical procedure was selected intraoperatively on the basis of diverticular morphology and disease severity including diverticular base width, suspected extension of ectopic tissue, degree of inflammation, and bowel viability.
LA-D was preferred for narrow-based diverticula without evidence of inflammation, ischemia, or suspected extension of ectopic mucosa into the adjacent ileum. LA-SBR was selected for broad-based diverticula, suspected ectopic mucosal involvement of the adjacent ileum, or complicated pathology such as inflammation, perforation, or ischemia.
All procedures were performed using a laparoscopic-assisted approach. The diverticulum or involved bowel segment was exteriorized through the umbilical incision before extracorporeal resection. For diverticulectomy, the diverticulum was resected extracorporeally with a linear stapler, and the staple line was oriented transversely to reduce the risk of luminal narrowing. For small bowel resection, segmental bowel resection followed by primary anastomosis was performed extracorporeally.
Participants
The study included patients who required either LA-D or LA-SBR with anastomosis, regardless of symptom status or the presence of complications such as bleeding, obstruction, or inflammation.
Variables
The exposure variable was the type of surgical procedure: LA-D or LA-SBR. The primary outcomes were operative time and postoperative hospital stay. Secondary outcomes were time to first oral feeding, postoperative complications, reoperation, and late complications during follow-up.
Data sources/measurement
Data were extracted from electronic medical records, operative notes, anesthesia records, pathology reports, and outpatient follow-up records. Operative time was defined as the interval from skin incision to wound closure. Time to first oral feeding was defined as the number of postoperative days until oral intake was initiated. Postoperative hospital stay was defined as the number of days from operation to discharge. Complications were identified from inpatient records and follow-up visits.
Bias
Because the surgical procedure was selected intraoperatively according to diverticular morphology, suspected ectopic mucosal extension, inflammation, and bowel viability, confounding by indication was possible. To reduce selection bias, all eligible consecutive patients during the study period were included, and baseline clinical characteristics were compared between groups. However, residual confounding from unmeasured anatomical or disease-severity factors could not be excluded.
Study size
No a priori sample size calculation was performed because Meckel diverticulum requiring surgery is uncommon, and this was a retrospective study including all eligible patients treated during the study period. Therefore, the analyses should be interpreted as exploratory, particularly for infrequent outcomes such as complications and reoperation.
Statistical analysis
Statistical analyses were conducted using IBM SPSS ver. 25.0 (IBM Corp.). Continuous variables were summarized as median (interquartile range [IQR]), and categorical variables were summarized as number (%). Between-group comparisons for continuous outcomes were performed using the Mann-Whitney U test, and effect sizes were additionally reported as Hodges-Lehmann estimates of location shift with 95% confidence intervals (CIs) where applicable. Categorical variables were compared using Fisher exact test or the chi-square test, as appropriate. Operative time analyses were conducted as complete-case analyses because operative time data were missing in cases with concomitant procedures; the number of available observations is reported for each group. A two-sided P-value <0.05 was considered statistically significant.
RESULTS
Baseline characteristics and perioperative outcomes are summarized in
Table 1 and
Fig. 1. A total of 39 patients underwent laparoscopic-assisted surgery for Meckel diverticulum, including 19 patients in the LA-D group and 20 in the LA-SBR group.
Baseline demographic characteristics were comparable between the two groups. The proportion of male patients was 89.5% in the LA-D group and 80.0% in the LA-SBR group (P=0.661). The median age at surgery was 10.0 years (IQR, 3.1–13.7 years) in the LA-D group and 5.8 years (IQR, 2.6–10.9 years) in the LA-SBR group (P=0.550). Median body weight at surgery was 42.0 kg (IQR, 12.5–55.1 kg) and 22.1 kg (IQR, 13.0–38.1 kg), respectively (P=0.351).
Preoperative clinical presentations were similar between groups. Gastrointestinal bleeding was the most common presentation (52.6% vs. 50.0%, P=0.869), followed by intestinal obstruction (15.8% vs. 35.0%, P=0.273). Severe intra-abdominal inflammation, including abscess formation, was observed in a small number of patients (5.3% vs. 10.0%, P=0.999). Six patients (15.4%) were asymptomatic at diagnosis, with a higher proportion in the LA-D group than in the LA-SBR group (26.3% vs. 5.0%, P=0.091).
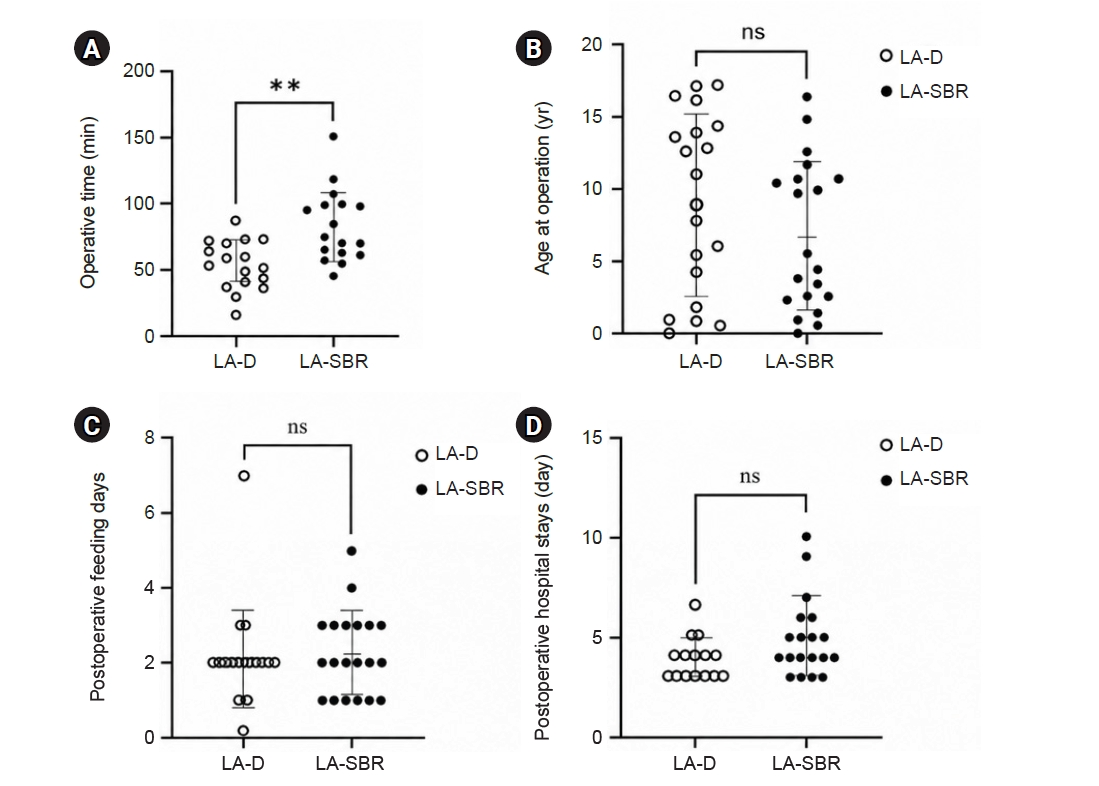
Operative outcomes showed a significantly shorter operative time in the LA-D group (n=15) than in the LA-SBR group (n=16) (median, 55.0 minutes vs. 76.0 minutes; P=0.002). Operative time data were available for 31 patients because data from eight cases were excluded (four in each group) owing to missing or nonseparable operative duration records, particularly in patients who underwent combined procedures with other surgical departments. The estimated difference in operative time between groups, assessed using the Hodges-Lehmann method, was 22.0 minutes (95% CI, 9.0–34.5 minutes) in the LA-SBR group.
Postoperative recovery outcomes were largely comparable. Time to first oral feeding did not differ significantly between groups (median, 2 days [2–2 days] vs. 2 days [1–3 days]; P=0.397). Postoperative hospital stay also did not differ significantly between the LA-D and LA-SBR groups (median, 4 days [3–4 days] vs. 4 days [4–5 days]; P=0.118), although the LA-SBR group showed a tendency toward longer hospitalization, with a Hodges-Lehmann location shift of 1.0 day (95% CI, 0–1.0 day).
Postoperative complications were infrequent in both groups (1 vs. 2 events), and no statistically significant difference was observed between groups (5.3% vs. 10.0%, P=0.999). However, because the number of events was very small, meaningful comparison between groups was limited. Two patients developed postoperative ileus requiring conservative management, and one patient in the LA-SBR group underwent reoperation for adhesive ileus.
Body weight was not significantly associated with operative time (Spearman ρ=0.21, P=0.24) or postoperative complications (P=0.550). Although body weight was numerically higher in the LA-D group than in the LA-SBR group, this difference was not statistically significant (P=0.351).
The median follow-up duration was 1.0 month (IQR, 0.5–7.8 months), with follow-up conducted through outpatient clinic visits. No late complications, including bowel stenosis or residual symptoms related to ectopic tissue, were observed during the follow-up period.
DISCUSSION
Key results
In this study, LA-D was associated with significantly shorter operative time and a tendency toward shorter postoperative hospital stay compared with LA-SBR, while early postoperative bowel recovery and complication rates were comparable between the two approaches.
Interpretation/comparison with previous studies
These findings are consistent with previous studies suggesting that diverticulectomy is associated with more favorable perioperative outcomes than segmental bowel resection [
5,
7].
These results are clinically relevant because they support a less extensive surgical strategy for appropriately selected patients with Meckel diverticulum. In the absence of high-risk features, diverticulectomy preserves the native bowel, avoids anastomosis, and reduces operative complexity, which may translate into faster recovery and shorter hospitalization. Previous literature has emphasized the advantages of minimally invasive approaches in reducing surgical trauma and improving postoperative recovery [
1,
4,
8].
The longer operative time and hospital stay observed in the LA-SBR group are likely attributable to the additional technical steps required for mesenteric division and bowel anastomosis. Segmental resection inherently involves more extensive tissue handling and reconstruction, which has been associated with increased postoperative morbidity in prior studies [
7,
9]. In contrast, diverticulectomy minimizes disruption of bowel continuity and may therefore contribute to improved perioperative outcomes.
Importantly, time to first oral feeding did not differ significantly between the two groups. This finding is consistent with reports that early bowel recovery may be similar after minimally invasive procedures [
1,
5].
A key consideration in interpreting these results is the potential for selection bias. The choice of surgical procedure was determined intraoperatively based on diverticular morphology and disease severity. Patients undergoing LA-SBR may have had more complex disease, such as broad-based diverticula or associated inflammation. Previous studies have also highlighted that diverticular characteristics, including base width and the presence of ectopic mucosa, play an important role in determining the appropriate surgical approach [
6,
10].
Although body weight showed a trend toward association with surgical approach selection, it was not significantly associated with operative time or postoperative complications, suggesting that body weight alone may not be a determining factor in surgical outcomes.
Clinical implication
These results support intraoperative selection of the procedure according to diverticular anatomy and disease severity. LA-D may be considered the initial surgical approach in cases with a narrow-based diverticulum without evidence of inflammation, ischemia, or suspected ectopic mucosal extension. Conversely, small bowel resection should be reserved for cases with high-risk features, including a broad base, involvement of the adjacent ileum, or complicated pathology such as perforation or severe inflammation. This approach is supported by previous reports emphasizing individualized surgical decision-making based on intraoperative findings [
3,
11-
13].
The absence of late complications, including bowel stenosis or residual symptoms related to ectopic tissue, further supports the safety of diverticulectomy in appropriately selected patients, although the short follow-up limits assessment of delayed adverse outcomes. Nevertheless, because incomplete resection of ectopic mucosa remains a concern, particularly in broad-based diverticula, careful intraoperative assessment is needed to reduce this risk [
6,
10].
This study has several limitations. Its retrospective design introduces inherent risks of selection bias and unmeasured confounding. The relatively small sample size limits the feasibility of robust multivariable analysis or propensity score matching. Additionally, operative time data were missing in a subset of patients, and the follow-up duration may not be sufficient to capture all late complications. Nevertheless, this study provides useful comparative data reflecting real-world clinical practice in the era of minimally invasive surgery.
Generalizability
The findings of this study are most applicable to patients with Meckel diverticulum treated at tertiary centers with experience in laparoscopic-assisted pediatric or adolescent surgery. Because this was a single-center retrospective study with a small sample size, the results should be generalized cautiously to other institutions, adult populations, open surgical approaches, purely intracorporeal laparoscopic procedures, or patients with severely complicated disease.
Suggestions for further studies
Future multicenter prospective registry studies are needed to validate these findings in larger and more diverse patient populations. Such studies should collect standardized intraoperative variables, including diverticular base width, diverticulum length, presence and location of ectopic mucosa, degree of inflammation, bowel viability, and the specific reason for selecting diverticulectomy or small bowel resection. Larger datasets would allow multivariable adjustment or propensity-score methods to reduce confounding by indication and provide more precise estimates of postoperative complications, reoperation, and long-term outcomes.
Conclusions
In this single-center retrospective cohort study, LA-D was associated with shorter operative time and a trend toward shorter postoperative hospital stay than LA-SBR, with no observed difference in time to first oral feeding or early postoperative complications. Because the surgical procedure was selected according to intraoperative findings and follow-up was limited, these findings support LA-D as a reasonable option for carefully selected patients with narrow-based, uncomplicated Meckel diverticulum, while small bowel resection remains appropriate for broad-based diverticula, suspected ectopic mucosal extension, ischemia, perforation, or severe inflammation.
NOTES
-
Authors’ contributions
Conceptualization: IAA, SP. Data curation: IAA, WK. Formal analysis: IAA, WK. Funding acquisition: JMS. Investigation: SL, JMS. Methodology: SL, SP. Project administration: SP. Supervision: SL, JMS, SP. Visualization: IAA. Validation: WK, SL, JMS. Writing–original draft: IAA, WK, SL, JMS, SP. Writing–review & editing: SP. All authors read and approved the final manuscript.
-
Conflict of interest
Sanghoon Lee is an editorial board member of this journal, but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
-
Funding
This work was supported by the SMC-Ottogi Research Fund (No. SMO1190231).
-
Data availability
All data generated or analyzed during this study are included in this published article. Additional data may be requested from the corresponding author.
Fig. 1.Comparison of selected perioperative outcomes between LA-D and LA-SBR. (A) Operative time in minutes (P=0.002); (B) age at operation; (C) time to first oral feeding; and (D) postoperative hospital stay. LA-D, laparoscopic-assisted diverticulectomy; LA-SBR, laparoscopic-assisted small bowel resection; ns, not significant. **P<0.01.
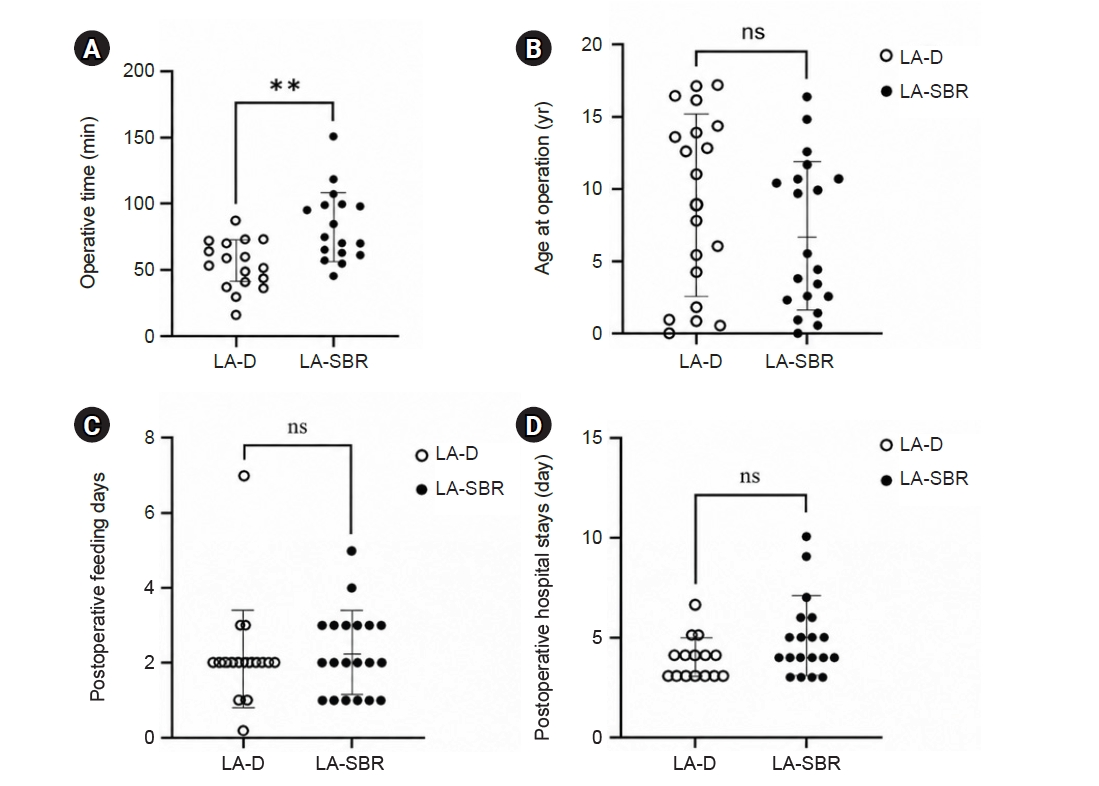
Table 1.Baseline characteristics and clinical outcomes
Table 1.
|
Characteristic |
Total (n=39) |
LA-D (n=19) |
LA-SBR (n=20) |
P-value |
|
Male sex |
33 (84.6) |
17 (89.5) |
16 (80.0) |
0.661 |
|
Age at operation (yr) |
7.8 (2.5–12.7) |
10.0 (3.1–13.7) |
5.8 (2.6–10.9) |
0.550 |
|
Weight at surgery (kg) |
28.3 (12.5–48.7) |
42.0 (12.5–55.1) |
22.1 (13.0–38.1) |
0.351 |
|
Preoperative symptoms |
|
|
|
|
|
Bleeding |
20 (51.3) |
10 (52.6) |
10 (50.0) |
0.869 |
|
Obstruction |
10 (25.6) |
3 (15.8) |
7 (35.0) |
0.273 |
|
Severe inflammation (abscess) |
3 (7.7) |
1 (5.3) |
2 (10.0) |
0.999 |
|
Asymptomatic |
6 (15.4) |
5 (26.3) |
1 (5.0) |
0.091 |
|
Operative time (min)a)
|
68.0 (55.5–83.5) |
55.0 (44.5–69.0) |
76.0 (66.0–99.5) |
0.002 |
|
Time to first oral feeding (day) |
2 (1.5–3.0) |
2 (2.0–2.0) |
2 (1.0–3.0) |
0.397 |
|
Postoperative hospital stays (day) |
4 (3.0–5.0) |
4 (3.0–4.0) |
4 (4.0–5.0) |
0.118 |
|
Complication |
3 (7.7) |
1 (5.3) |
2 (10.0) |
0.999 |
|
Ileus (conservative management) |
2 (5.1) |
1 (5.3) |
1 (5.0) |
0.999 |
|
Reoperation (adhesive ileus) |
1 (2.6) |
0 (0) |
1 (5.0) |
0.999 |
|
Follow-up (mo) |
1.0 (0.5–7.8) |
0.6 (0.5–5.0) |
1.3 (0.5–10.5) |
0.985 |
REFERENCES
- 1. Jung HS, Park JH, Yoon SN, Kang BM, Oh BY, Kim JW. Clinical outcomes of minimally invasive surgery for Meckel diverticulum: a multicenter study. Ann Surg Treat Res 2020;99:213-20.
- 2. Sagar J, Kumar V, Shah DK. Meckel’s diverticulum: a systematic review. J R Soc Med 2006;99:501-5.
- 3. Sharma RK, Jain VK. Emergency surgery for Meckel’s diverticulum. World J Emerg Surg 2008;3:27.
- 4. Kasem HM, Alekrashi M, Elshahat W. Laparoscopy-assisted approach for Meckel’s diverticulum in pediatric age. World J Lap Surg 2020;13:65-8.
- 5. Redman EP, Mishra PR, Stringer MD. Laparoscopic diverticulectomy or laparoscopic-assisted resection of symptomatic Meckel diverticulum in children?: a systematic review. Pediatr Surg Int 2020;36:869-74.
- 6. Can M, Ergin M, Okur O, Payza AD, Polatdemir K, Oral A. Can deciphering the growth of Meckel's diverticulum help us to decide the resection technique? Front Surg 2024;11:1421732.
- 7. Brungardt JG, Cummiskey BR, Schropp KP. Meckel’s diverticulum: a National Surgical Quality Improvement Program survey in adults comparing diverticulectomy and small bowel resection. Am Surg 2021;87:892-6.
- 8. Skertich NJ, Ingram MC, Grunvald MW, et al. Outcomes of laparoscopic versus open resection of Meckel's diverticulum. J Surg Res 2021;264:362-7.
- 9. Cullen JJ, Kelly KA, Moir CR, Hodge DO, Zinsmeister AR, Melton LJ. Surgical management of Meckel’s diverticulum: an epidemiologic, population-based study. Ann Surg 1994;220:564-8.
- 10. Shin HW, Kang YN, Park J. Clinicopathologic characteristics and treatment outcomes of symptomatic Meckel’s diverticulum in children. Adv Pediatr Surg 2021;27:8-14.
- 11. Ruscher KA, Fisher JN, Hughes CD, et al. National trends in the surgical management of Meckel’s diverticulum. J Pediatr Surg 2011;46:893-6.
- 12. Tree K, Kotecha K, Reeves J, et al. Meckel’s diverticulectomy: a multi-centre 19-year retrospective study. ANZ J Surg 2023;93:1280-6.
- 13. Alemayehu H, Stringel G, Lo IJ, et al. Laparoscopy and complicated Meckel diverticulum in children. JSLS 2014;18:e2014.00015.