

Purpose
To report the clinical progress and findings seen in pediatric airway surgeries performed by a single pediatric surgeon.
Methods
We retrospectively reviewed 32 pediatric patients with various airway diseases who underwent surgical correction performed by a single pediatric surgeon between January 2005 and March 2021. Surgical indications depended on the presence and severity of respiratory symptoms. Surgical results were considered good if symptoms improved and normal respiration was possible without dependence on a ventilator or tracheostomy, without postoperative complications, at the last postoperative follow-up.
Results
A total of 32 patients who underwent airway surgery were diagnosed with 3 types of surgical airway diseases: tracheomalacia (n=19), subglottic stenosis (n=10), and tracheal stenosis (n=3). In the treatment for tracheomalacia, surgical efficacy was 88.2% for aortopexy and 100.0% for tracheopexy. The postoperative mortality rate of slide thyrocricotracheoplasty for subglottic stenosis and slide tracheoplasty for tracheal stenosis was 20.0%. The age at the time of all airway surgeries ranged from 1.0 to 127.6 months (median, 4.8 months). The postoperative follow-up period ranged from 1.2 months to 16.6 years (median, 4.5 years).
Conclusion
Severe pediatric airway diseases with obstructive symptoms are life-threatening and require surgical treatment. Pediatric airway surgery performed in this study by a single pediatric surgeon had similar or better outcomes than in previous studies. However, more accurate diagnostic methods and improved surgical procedures for pediatric airway diseases require development.
To report the clinical progress and findings seen in pediatric airway surgeries performed by a single pediatric surgeon.
We retrospectively reviewed 32 pediatric patients with various airway diseases who underwent surgical correction performed by a single pediatric surgeon between January 2005 and March 2021. Surgical indications depended on the presence and severity of respiratory symptoms. Surgical results were considered good if symptoms improved and normal respiration was possible without dependence on a ventilator or tracheostomy, without postoperative complications, at the last postoperative follow-up.
A total of 32 patients who underwent airway surgery were diagnosed with 3 types of surgical airway diseases: tracheomalacia (n=19), subglottic stenosis (n=10), and tracheal stenosis (n=3). In the treatment for tracheomalacia, surgical efficacy was 88.2% for aortopexy and 100.0% for tracheopexy. The postoperative mortality rate of slide thyrocricotracheoplasty for subglottic stenosis and slide tracheoplasty for tracheal stenosis was 20.0%. The age at the time of all airway surgeries ranged from 1.0 to 127.6 months (median, 4.8 months). The postoperative follow-up period ranged from 1.2 months to 16.6 years (median, 4.5 years).
Severe pediatric airway diseases with obstructive symptoms are life-threatening and require surgical treatment. Pediatric airway surgery performed in this study by a single pediatric surgeon had similar or better outcomes than in previous studies. However, more accurate diagnostic methods and improved surgical procedures for pediatric airway diseases require development.
Pediatric airway disease to congenital, acquired, or iatrogenic causes affects the larynx, trachea, and bronchus. Tracheomalacia and tracheal stenosis are the most common congenital abnormalities of the pediatric airway [1]. Although many cases improve with conservative treatment, those requiring surgical treatment can be severe and have high mortality rates without immediate treatment [1, 2, 3, 4]; hence, the required involvement of pediatric surgeons. Tracheomalacia associated with esophageal atresia is an example of such cases. Tracheomalacia is typically detected incidentally upon managing or operating on patients with esophageal atresia [5, 6, 7]. Pediatric airway disease has a broad spectrum of symptoms and requires careful diagnosis. Challenging cases require collaboration among specialists such as pediatric surgeons, pediatricians, radiologists, pediatric otolaryngologists, pediatric thoracic surgeons, and anesthesiologists. Currently, increasing interest in pediatric airway surgery arises from increased global reports from pediatric surgeons. However, few reports are available on airway surgeries performed by pediatric surgeons in Korea. Hence, this study aimed to report the clinical progress and surgical findings in patients who underwent pediatric airway surgery performed by a single pediatric surgeon in Korea.
Between January 2005 and March 2021, 32 pediatric patients with various airway diseases underwent surgical treatment by a single pediatric surgeon. We retrospectively reviewed the medical records of the 32 patients following approval from the institutional review board (IRB) of Severance Hospital (IRB No. 4-2021-1740) in accordance with the Helsinki Declaration. Patient demographics, pre- and postoperative clinical symptoms, airway evaluation, surgical techniques, and outcomes were determined.
All patients underwent diagnostic bronchoscopy or chest computed tomography (CT). Flexible or rigid bronchoscopy was performed to visually evaluate airway disease features (tracheal cartilage shape, collapse, or narrowing pattern) and extent of the airway lesions. In addition, chest CT images were obtained to study associated mediastinal cardiovascular anomalies, tracheal diverticula, peripheral bronchi, and lung parenchyma.
Surgical indication depended on the presence and severity of respiratory symptoms, anoxic spells, intermittent respiratory obstruction, and dependence on endotracheal tube intubation or tracheostomy (Table 1). Surgical results were considered good if the following conditions were achieved: 1) improvement of symptoms, 2) achievement of normal respiration without dependence on a ventilator or tracheostomy, and 3) lack of postoperative complications at the last follow-up after surgery. Postoperative complications were defined as any complication greater than grade III in the Clavien-Dindo classification that required intensive care unit admission, warranted intervention, and required re-operation [8].

Table 1
Surgical indications
All statistical analyses were performed using IBM SPSS Statistics ver. 26.0 (IBM Co., Armonk, NY, USA).
A total of 32 patients who underwent airway surgery were diagnosed with 3 types of operative airway diseases: tracheomalacia, subglottic stenosis, and tracheal stenosis (Table 2). Nineteen patients were diagnosed with congenital tracheomalacia, and 14 (73.7%) of them were male. Seventeen patients with tracheomalacia (89.5%) had a history of corrective surgery for esophageal atresia (gross type C) and 12 patients (63.2%) had other anomalies. Of the 10 patients with subglottic stenosis, 6 (60.0%) were congenital and 4 (40.0%) were acquired. Five patients (50.0%) with subglottic stenosis were male. Among the patients with acquired subglottic stenosis, 2 were due to trauma, and 2 were due to iatrogenic causes. Two patients with subglottic stenosis (20.0%) had a history of corrective surgery for esophageal atresia (gross type C), and 5 patients (50.0%) had other anomalies. All 3 patients with tracheal stenosis had congenital type disease, were male, and had accompanying anomalies. The age at the time of all airway surgeries ranged from 1.0 to 127.6 months (median, 4.8 months).

Table 2
Clinical characteristics of the patients who underwent airway surgery
The operation types and postoperative outcomes of airway surgery are shown in Table 3. Of the 19 patients with tracheomalacia, 17 underwent aortopexy (15 open, 2 thoracoscopic) and all had a history of esophageal atresia (gross type C) surgery. Among the 15 patients who underwent open aortopexy, 3 underwent preoperative tracheostomy or intubation due to respiratory difficulty. Of these, 2 patients required tracheostomy due to delayed extubation during the immediate postoperative period, and one patient improved enough to extubate with sealing off the tracheostomy later. Postoperative complications occurred in 2 patients who underwent open aortopexy. One patient developed pneumonia with sepsis and was admitted to the intensive care unit for a prolonged postoperative period and maintained on tracheostomy at the last follow-up. The other patient developed recurrent pneumonia, and at follow-up, developed a respiratory arrest event secondary to airway obstruction, which required the initiation of advanced cardiovascular life support and intensive care unit admission.
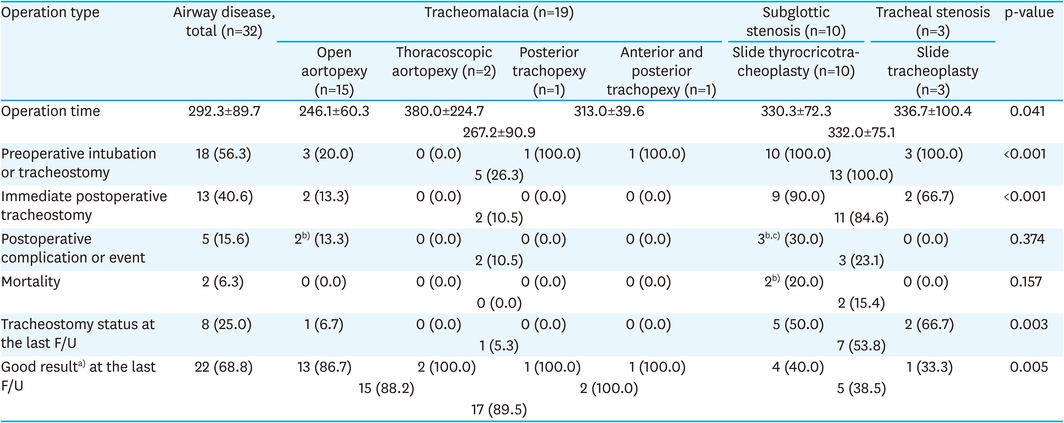
Table 3
Operation types and postoperative outcomes of airway surgery
Conversely, 2 patients who underwent thoracoscopic aortopexy did not undergo preoperative tracheostomy or intubation and showed good results without postoperative tracheostomy or complications. Of the 19 patients with tracheomalacia, 2 underwent tracheopexy through posterior muscle-sparing right thoracotomy (one, posterior tracheopexy) or a lower cervical incision (one, anterior and posterior tracheopexy), and none had a history of esophageal atresia (gross type C) surgery. Preoperative intubation was performed in both patients due to respiratory difficulty, but achieved good postoperative results.
All 10 patients with subglottic stenosis underwent slide thyrocricotracheoplasty [9, 10], and 3 patients with tracheal stenosis underwent slide tracheoplasty. Due to respiratory difficulties, all patients with subglottic and tracheal stenosis underwent preoperative tracheostomy or intubation. During the immediate postoperative period, 9 patients who underwent thyrocricotracheoplasty and 2 who underwent tracheoplasty underwent postoperative tracheostomy due to delayed extubation. Of these, only 4 patients who underwent thyrocricotracheoplasty improved enough to extubate with sealing off tracheostomy later, and the remaining 7 patients were maintained on tracheostomy at the last follow-up.
Postoperative complications occurred in 3 patients who underwent slide thyrocricotracheoplasty. One patient experienced a methicillin-resistant Staphylococcus aureus (MRSA) infection of the tracheal cartilage at the anastomosis site of the thyrocricotracheoplasty, leading to acute anastomosis disruption of the airway with respiratory arrest. The following day, the patient underwent end-to-end re-anastomosis surgery, and tracheostomy was performed after extensive debridement of the infected necrotic tissue around the anastomotic site. The patient did not show good results because of the complication but improved after extubation and sealing off the tracheostomy during the follow-up period. Another patient experienced refractory pneumonia with sepsis and expired 37 days after surgery. Further, during the follow-up period, one patient experienced respiratory arrest secondary to airway obstruction, which progressed to brain death.
The postoperative follow-up period ranged from 1.2 months to 16.6 years (median, 4.5 years). There was a statistically significant difference between tracheomalacia and subglottic and tracheal stenosis. Patients with tracheomalacia had a significantly shorter operation time than those with subglottic and tracheal stenosis (267.2 vs. 332.0 minutes; p=0.041). In addition, there were significant differences in the results of preoperative intubation or tracheostomy (p<0.001), immediate postoperative tracheostomy (p<0.001), and tracheostomy status at the last follow-up (p=0.003). Moreover, good results at the last follow-up showed statistically significant differences (p=0.005).
Statistically significant correlations were observed between the preoperative intubation or tracheostomy status and immediate postoperative tracheostomy (p<0.001), and between preoperative intubation or tracheostomy status and poor postoperative outcomes (p=0.019) (Table 4).

Table 4
Correlation between preoperative intubation or tracheostomy status and postoperative outcomes
Pediatric airway disease incidence is varied and underestimated. As diagnosis is difficult, some severe cases may result in early infant death [1]. Previous reports have shown that the overall prevalence of congenital airway malformations is estimated between 1 in 10,000 and 1 in 64,500 births [11, 12].
Additionally, the high prevalence of airway disease in patients affected by esophageal atresia and the importance of early diagnosis and aggressive management has been demonstrated [13, 14]. Common embryology may explain the association between airway anomalies and esophageal atresia [7, 13, 14]. In the present study, the prevalence of airway disease associated with esophageal atresia was 59.4% (tracheomalacia 89.5%, subglottic stenosis 20.0%), comparable with other reports [13, 14]. Pediatric surgeons who frequently encounter esophageal atresia should place special focus on airway disease.
Pediatric airway disease causes various respiratory symptoms due to airway narrowing, such as exertional dyspnea, respiratory distress with cyanosis, apnea, acute life-threatening events, or repeated and prolonged infection. These symptoms are directly related to the degree of lumen narrowing and stenotic length. Invasive treatment of patients with mild symptomatic pediatric airway disease is controversial. However, severe pediatric airway disease with obstructive symptoms is life-threatening and requires invasive treatment such as emergency tracheostomy. Severe tracheomalacia has been reported to have a mortality rate of 80%, while severe congenital tracheal stenosis has the highest mortality rate (nearly 100%) [4, 12].
Although tracheostomy is life-saving in severe pediatric airway disease, it presents a risk of sudden death, recurrent infections, equipment failure, and tracheostomy-related complications [15, 16]. Various surgical techniques have been developed to treat pediatric airway diseases with increasing rates of operative success [7, 10, 12, 17, 18, 19, 20, 21]. Regardless of the approach or technique used, the efficacy of aortopexy for tracheomalacia was reportedly high (over 80%) in recent literature [18, 22]. Further, reported mortality rates after slide tracheoplasty for congenital tracheal stenosis were 12%–30% [21, 23]. It is predicted that these surgical techniques will be further developed to achieve better results.
Based on the present study results, surgical outcomes were similar to or better than those reported in other studies, although definitions vary in the literature. For the treatment of tracheomalacia, surgical efficacy was 88.2% for aortopexy and 100.0% for tracheopexy. In slide thyrocricotracheoplasty for subglottic stenosis and slide tracheoplasty for tracheal stenosis, the postoperative mortality rate was 20.0%. Few studies have directly evaluated the surgical efficacy of slide thyrocricotracheoplasty or slide tracheoplasty; therefore, comparisons could not be made.
This study showed a statistically significant difference in postoperative outcomes between tracheomalacia and subglottic and tracheal stenosis, which can be attributed to differences in surgical method and difficulty. Compared to surgery for tracheomalacia using aortopexy or tracheopexy, surgery for subglottic and tracheal stenosis with tracheoplasty accompanied by tracheal anastomosis is more complex and higher risk. Although no literature directly compares the results of the 2 surgical methods, the differences in operation time in this study are supportive.
In addition, preoperative intubation or tracheostomy status had a statistically significant effect on immediate postoperative tracheostomy and poor outcomes. Preoperative intubation or tracheostomy status may reflect the patient’s poor preoperative status, which affects the postoperative outcome. However, in this study, a comparison between preoperative intubation or tracheostomy status and preoperative status was not performed.
Bronchoscopy or chest CT was performed for postoperative structural evaluation in all patients who underwent pediatric airway surgery and confirmed the resolution of these structural problems at the surgical site. However, as shown in the results, symptoms did not improve in any patient postoperatively. This may have been due to physiopathological problems observed in bronchomalacia, bronchopulmonary dysplasia, and respiratory distress syndrome, which cannot be corrected surgically.
There is no consensus on treatment protocols or guidelines for pediatric airway diseases. Owing to the rarity of the disorder, various treatments have been reported in the literature as part of single case reports or small series of patients. Pediatric surgeons worldwide are committed to increasing the success rate of surgical treatment for pediatric airway diseases [7, 10, 18, 19, 20, 22, 24, 25, 26].
In conclusion, severe pediatric airway disease with obstructive symptoms is life-threatening and requires surgical treatment. However, definitive diagnosis and treatment may be delayed due to the rarity of the disorder and pediatric surgeons’ unfamiliarity. Nevertheless, surgical outcomes reported by a single pediatric surgeon in this study were on par with or better than those previously reported. Further studies are necessary to improve the diagnosis and treatment of pediatric airway diseases requiring surgical treatment; hence, we recommended extensive multicenter prospective studies.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: H.S.J.
Data curation: I.K., H.I.G.
Formal analysis: J.H.J.
Investigation: J.H.J.
Methodology: J.H.J.
Project administration: H.S.J.
Resources: I.K., H.I.G.
Software: J.H.J.
Supervision: H.S.J.
Validation: H.S.J.
Visualization: I.K., H.I.G.
Writing - original draft: J.H.J.
Writing - review & editing: H.S.J.
