

This study aimed to compare the outcomes of open fundoplication (OF) and laparoscopic fundoplication (LF) in children with gastroesophageal reflux disease (GERD).
We retrospectively reviewed the electronic medical charts of pediatric patients who underwent fundoplication for GERD between January 2005 and May 2018 at the Korean tertiary hospital. Patient characteristics, operation type, associated diagnosis, operation history, neurologic impairment, postoperative complication, recurrence, and operation outcomes were investigated. The Mann-Whitney U test or Student's t-test was used to evaluate continuous data as appropriate. The χ2 test was used to analyze categorical data.
A total of 92 patients were included in this study; 50 were male and 42 were female. Forty-eight patients underwent OF and 44 patients underwent LF. Patient characteristics, such as sex ratio, gestational age, symptoms, neurological impairment, and history of the previous operation were not different between the two groups. A longer operative time (113.0±56.0 vs. 135.1±49.1 minutes, p=0.048) was noted for LF. There was no significant difference in operation time when the diagnosis was limited to only GERD, excluding patients with other combined diseases. Other surgical outcomes, such as intraoperative blood loss, transfusion rate, hospital stay, and recurrence rate were not significantly different between the 2 groups. The complication rate was slightly higher in the OF group than in the LF group; however, the difference was not significant (20.8% vs. 11.4%, p=0.344).
LF is as safe, feasible, and effective as OF for the surgical treatment of GERD in children.
Anorectal duplications account for only 5% of gastrointestinal duplications, and cases with involvement of the anal canal are much rarer. Nearly all anorectal duplications are posterior to the rectum; duplications located anterior to the normal rectum are highly unusual, and only a few cases have been reported. We report the case of an anterior anorectocolonic duplication presenting as a rectovaginal fistula in a 2-month-old infant. After diagnosis, the duplication was excised completely without further intestinal complications.
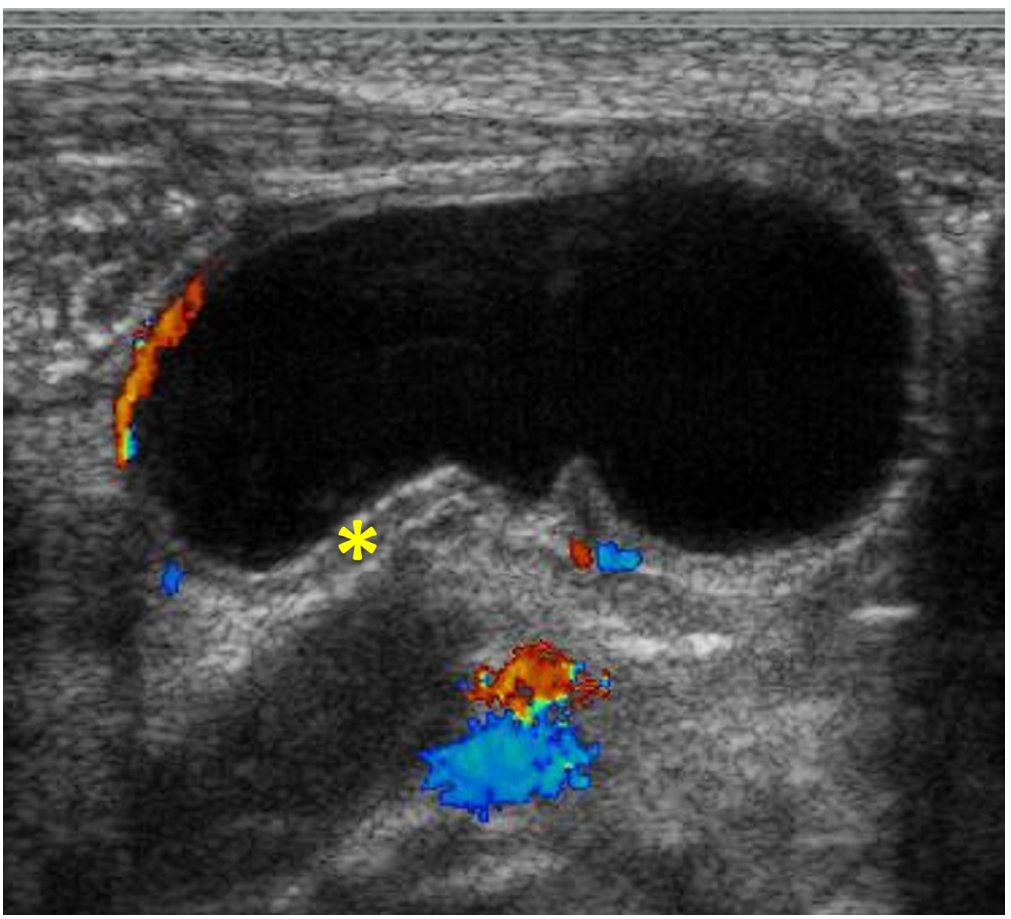
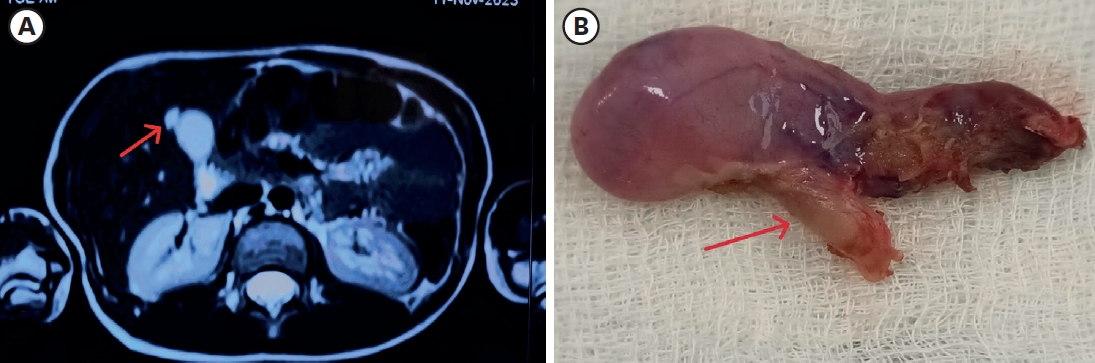
We report a neonatal case of “intraluminal” pyloric duplication cyst, causing gastric obstruction after birth. Endoscopy revealed a submucosal cystic lesion approximately 15 mm in size arising from the anterior and inferior surfaces of the pylorus obliterating the pyloric canal. After laparotomy, intraoperative cholangiography was performed, which documented no communication between the cyst and the bilio-pancreatic duct. Gastrotomy was performed transversally over the antrum, and the cyst delivered through the incision. The cyst was incised, the upper part of the cyst wall removed, and a mucosectomy performed on the inner cyst wall of the lower part. The mucosa and muscle of the margin of the cyst were approximated. At follow up of 10 months, the patient is well without any sign of gastric obstruction.
Citations
This study aimed to assess the long-term clinical outcome of laparoscopic Nissen fundoplication (LNF) in children according to their neurologic status.
The study retrospectively analyzed the data of 82 children (62 neurologically impaired and 20 neurologically normal children with primary gastroesophageal reflux disease) who had undergone LNF between 2003 and 2012. The main outcome measures were the occurrence of recurrence that required reoperation and post-procedure complications such as infections, pneumonia, and gastrointestinal complications including ileus, dysphagia, and delayed gastric emptying.
The median age at the time of the LNF was 25 months (range, 1-192 months), and the median of body weight was 10.0 kg (range, 2.8-37.0 kg). The average weight gain was 1.55±1.68 kg at 6 months, 3.32±2.30 kg at 1 year, and 5.63±4.22 kg at 2 years after surgery. Six (9.7%) of the 62 neurologically impaired patients and two (10.0%) of neurologically normal lost their body weight or had no weight changes. Eight (12.9%) of the 62 neurologically impaired children had required redo surgery because of gastroesophageal reflux disease recurrences, while 2 (10.0%) of the 20 neurologically normal children had experienced recurrences. In the neurologically impaired children, the postoperative complications included pneumonia (n=1), wound infection (n=1), urinary tract infection (n=1), dysphagia (n=1), delayed gastric emptying (n=1), and ileus (n=2). All of these complications were not found in the neurologically normal group, except for only one case of infectious colitis. However, there was no statistically significant difference between the two groups in postoperative complications.
The outcomes of laparoscopic fundoplication were similar in the neurologically impaired children and in the neurologically normal children.
The duplication of gastrointestinal tract has been known to be a rare condition and two different forms, cystic and tubular type. This study was conducted to examine its clinical characteristics, especially cystic enteric duplication which was detected antenatally or postnatally.
There were 13 patients, who confirmed as cystic enteric duplication after operation between July 1996 and June 2015. Clinical data, including a gender, age at operation, presenting symptoms, diagnostic modalities, locations of lesion, and results of surgical treatment, were reviewed retrospectively according to cases detected antenatally and postnatally.
Five cases were included in antenatal diagnosis group and 8 cases in postnatal diagnosis group. Both groups show slightly common in female and the lesion most common in ileum. Antenatal diagnosis group shows 2 males and 3 females and the mean age at operation was 12±52 days (range, 5 to 90 days). They received operation regardless of symptom. Postnatal group shows 3 males and 5 females and the mean age at operation was 462.5±777.0 days (range, 4 days to 6 years). Moreover, 6 patients (75.0%) were age before 2 years. They usually presented abdominal pain with vomiting.
Cystic enteric duplication could present symptoms at any time during childhood, mainly before 2 years old, and so a proper management should be considered when suspect it. Although it is uncommon, surgical management including a minimal invasive procedure could be attempted despite the neonatal period.
Laparoscopic appendectomy (LA) has become a gold standard for children even in complicated appendicitis. The purpose of this study was to compare the postoperative surgical site infection rates between laparoscopic and open appendectomy (OA) group in pediatric complicated appendicitis.
A total of 1,158 pediatric patients (age ≤15 years) underwent operation for appendicitis over a period of 8 years. Among these patients, 274 patients (23.7%) were diagnosed with complicated appendicitis by radiologic, operative and pathologic findings, and their clinical outcomes were retrospectively analyzed.
Of the 274 patients with complicated appendicitis, 108 patients underwent LA and 166 patients underwent OA. Patients in the LA group returned to oral intake earlier (1.9 days vs. 2.7 days; p<0.01) and had a shorter hospital stay (5.0 days vs. 6.3 days; p<0.01). However, rate of postoperative intra-abdominal infection (organ/space surgical site infection) was higher in the LA group (LA 15/108 [13.9%] vs. OA 12/166 [7.2%]; p<0.01). Readmission rate was also higher in the LA group (LA 9/108 [8.3%] vs. OA 3/166 [1.8%]; p<0.01).
The minimally invasive laparoscopic technique has more advantages compared to the open procedure in terms of hospital stay and early recovery. However, intra-abdominal infection and readmission rates were higher in the laparoscopy group. Further studies should be performed to evaluate high rate of organ/space surgical infection rate of laparoscopic procedure in pediatric complicated appendicitis.
Citations
Laparoscopic surgery has become popular in the past few decades, owing to less postoperative pain, fast recovery, and better cosmetic outcomes. The laparoscopic approach has been employed in pediatric surgery for the same reasons. After the first attempts of single incision laparoscopic appendectomy in pediatrics in 1998, single incision laparoscopic surgery (SILS) has recently been proven to be safe and feasible for the pediatric population. However, limitations have been reported for SILS, such as the wide learning curve, compared to standard laparoscopic surgery, and the restricted number of hospitals with surgical training programs including SILS. In this study, we intend to present our initial experiences with SILS in children, and to describe the technique, instruments used, and outcomes. This is a retrospective study of 71 pediatric patients who underwent SILS, at a tertiary medical center, between September, 2012 and August, 2013. Electronic medical records were reviewed for demographics, type of procedure, operation time, use of additional ports, conversion to open surgery, complications and hospital stay. Additional ports were inserted in 4 cases, for the purpose of traction. Postoperative complications were noted in 13 cases, which were mostly related to wound inflammation or formation of granulation tissue. According to our analyses, patients with complications had significantly longer use and more frequent use of pain killers. Notwithstanding the small sample size, many of the procedures performed in pediatric patients seem to be possible with SILS.
Citations
Fundoplication is a common surgical procedure for gastroesophageal reflux Disease (GERD). Recently the procedure has been performed with increased frequency laparoscopically. The aim of this study is to compare laparoscopic Nissen fundoplication (LNF) and open Nissen fundoplication (ONF) for GERD in children. We studied retrospectively the 88 pediatric patients who underwent the Nissen fundoplication for GERD as primary antireflux surgery from 1994 and 2009. ONF was performed in 34 cases and LNF was in 54 cases. 58 patients have neurologic impairment. Time to initial food intake after the surgery were reduced in the LNF group (
Gastric duplication is a rare anomaly which account for only 3.8% of all gastrointestinal duplication. Gastric duplications are usually cysticlesion without communication with lumen. Most frequent presentation is an abdominal mass with vomiting, mainly diagnosed within the first year of life. Surgical removal is necessary in all cases, and optimal timing for surgery is the time that diagnosis is made. However, prenatally diagnosed gastric duplication is getting more common, and determining timing for surgery is not easy due to absent or minimal symptoms just after birth. We experienced prenatally diagnosed gastric duplication in a female newborn baby that gastric duplication was suggested in 24th week of gestational age through prenatal ultrasonogram. Surgical removal was done at 3 months after birth, and showed good results. We think that natural history of gastric duplication and prevalent age of surgical disease which is similar to gastric duplication such infantile hypertrophic pyloric stenosis should be considered when timing of surgery on prenatally gastric duplication is decided.
Delayed gastric emptying (DGE)commonly occurs after Nissen fundoplication in patients with gastroesophageal reflux disease. Since the understanding of its pathogenesis is insufficient, an effective method of management has not yet been suggested. The authors report a case of a 16-year-old girl with DGE after laparoscopic Nissen fundoplication and treated with intravenous injection of low dose erythromycin.
Abdominal cerebrospinal fluid pseudocyst is an uncommon complication of ventriculoperitoneal shunt (VPS) performed for hydrocephalus. The incidence of VPS complications in children is higher than in adults. There are controversies and difficulties in the treatment of the abdominal pseudocyst. We report a case of abdominal pseudocyst complicating VPS in a boy. Partial excision of pseudocyst and replacement of the VP shunt were effective during a followup of 18 months postoperatively with no recurrence.
Hickman catheters are tunneled central venous catheters used for long-term venous access in children with malignancies. The appropriate management for various kinds of catheter related complications has become a major issue. We retrospectively analyzed the clinical, demographic, and surgical characteristics in 154 pediatric hemato-oncology patients who underwent Hickman catheter insertion between January 2005 and December 2009. There were 92 boys and 62 girls. The mean age at surgery was 7.6±5.1 years old. The mean operation time was 67.4±21.3 minutes and C-arm fluoroscopy was used in 47(30.5%). The causes of Hickman catheter removal were termination of use in 82 (57.3%), catheter related bloodstream infection in 44(30.8%), mechanical malfunction in 11(7.7%), and accidents in 6(4.2%). Univariate and multivariate analysis for associated factors with catheter related bloodstream infection showed that there were no statistically significant associated factors with catheter related infection complications. All cases except two showed clinical improvement with catheter removal and relevant antibiotics treatment. The mean catheter maintenance period in patients of catheter removal without complications was 214.9±140.2 days. And, The mean catheter maintenance period in patients of late catheter related bloodstream infection was 198.0±116.0 days. These data suggest that it is important to remove Hickman catheter as soon as possible after the termination of use. When symptoms and signs of complications were noticed, prompt diagnostic approach and management can lead to clinical improvements.
Catheter related and perianal problems are common surgical complications encountered during the treatment of pediatric malignancies. However acute surgical abdominal emergencies are rare. The aim of this study is to review acute surgical abdominal complications that occur during the treatment of childhood malignancies. Out of a total of 1,222 patients who were newly diagnosed with malignant disease, between January 2003 and May 2008, there were 10 patients who required surgery because of acute abdominal emergencies. Their medical records were reviewed retrospectively. Hematologic malignancies were present in 7 patients (4 leukemia, 2 lymphoma, 1 Langerhans cell histiocytosis) and solid tumors in 3 patients (1 adrenocortical carcinoma, 1 desmoplastic small round cell tumor, 1 rhabdomyosarcoma). Seven patients had intestinal obstruction, two had gastrointestinal perforation and one, typhlitis. Intestinal obstructions were treated with resection of the involved segment with (N=2) or without (N=3) enterostomy. Two patients had enterostomy alone when resection could not be performed. Intestinal perforation was treated with primary repair. Typhlitis of the ascending colon was treated with ileostomy. Right hemicolectomy was necessary the next day because of the rapidly progressing sepsis. Three patients are now alive on chemotherapy and one patient was lost to followed-up. Among six patients who died, five died of their original disease progression and one of uncontrolled sepsis after intestinal perforation. Although rare, acute surgical abdominal complications can occur in childhood malignancies. Rapid and accurate diagnosis and appropriate operation are required for effective treatment of the complications.
Children who underwent reparative operations for esophageal atresia (EA) with or without tracheoesophageal fistula (TEF), are confronted with many gastrointestinal or respiratory problems, especially during the early years of life. We reviewed the medical records of 50 patients who underwent repairs of EA with or without TEF at the Division of Pediatric Surgery, Samsung Medical Center, from December 1994 to December 2005. Current status of children was accessed by telephone-interview, but only 27 of them were accessible. Of 50 patients, 3 patients (6%) were type A, 45 patients (90%) were type C, and 2 patients (4%) were type E. The mean interval between primary operation and interview was 5.5 years. The incidences of growth retardation (<10 percentile of height/weight) were 39% and 21 % during the first 5 years after repairs, respectively. The incidences of dysphagia or gastroesophageal reflux and recurrent respiratory infections were 33% and 39 %, respectively. However, these problems were likely to improve as the children grew. The incidences of growth retardations (<10 percentile of height/weight) were 11% and 11% for the children more than five years postoperative. The incidences of dysphagia or gastroesophageal reflux and recurrent respiratory infections were 22% and 22%, respectively. Children with EA with or without TEF are faced with many obstacles. Close observation and adequate treatment for delayed postoperative complications are necessary to improve the quality of life for these children.
Citations
Fundoplication is a common surgical procedure for gastroesophageal reflux disease (GERD). Recently the procedure has been performed with increased frequency laparoscopically. The aim of this study is to review our 11 years experience with fundoplication in infants and children. From October 1994 to December 2005, 59 fundoplications in 55 patients were performed at Sungkyunkwan University Samsung Medical Center. Medical records and laboratory results of these children were retrospectively reviewed for sex, age, symptoms and signs, coexisting disease, diagnostic methods, treatment modalities and length of operative time. Open fundoplication was performed in 41 cases and laparoscopic fundoplication in 18 cases. Simultaneous gastrostomy was done in 27 cases. Recurrent GERD symptom occurred in four patients (7.2 %) within 2 years after first fundoplication and all 4 patients had re-do fundoplication. There were no intra- and immediate post-operative complications. Gastrointesitnal symptoms were the most common indication for fundoplication in neurologically normal patients. The most frequent diagnostic studies were upper gastrointestinal series (76.3 %) and 24 hour esophageal pH monitoring (78.2 %). Fundoplication had been increased since 2004 and mostly done laparoscopically. In conclusion, our 11 years' practice of open and laparoscopic fundoplication indicates that both approaches are safe and effective in the treatment of GERD for infants and children.
Citations
The aim of this study is to analyze the outcomes of the esophageal atresia with tracheoesophageal fistula over the last 2 decades. The records of 51 patients born between 1987 and 2006 were reviewed. Twenty-seven patients were male. Mean values of the age, gestational age and birth weight were 2.9 days, 296 days and 2.7kg, respectively. All patients had Gross type C anomalies. Thirty-one patients (60.7 %) had one or more associated congenital anomalies and the most common anomaly was cardiac malformation. In 48 cases, primary anastomosis was done and staged operation was done in one case. Circular myotomies in the proximal esophagus were performed in 9 cases. Postoperative complication developed in 26 cases (54 %): pulmonary complication in 12 cases, anastomotic leakage in 10 and anastomotic stricture in 10, recurrent trachoesophageal fistula in one and tracheomalasia in 2 cases. Reoperation was carried out in 2 patients with anastomotic leaks, the remaining leaks were managed non operatively. Three of the strictures were reoperated upon and the others were successfully managed by balloon dilatations. Overall mortality rate was 15.6 %. Mortality rate of the second 10 years (8 %) period decreased significantly compared to that of the first 10 years (23 %) period.
Citations
Meckel's diverticulum is the most common congenital anomaly of gastrointestinal tract in children. The incidence of complicated Meckel's diverticulum is about 4%. The major complications of Meckel's diverticulum are bleeding, intussusception, obstruction and perforation. The aim of this study was to investigate the clinical manifestations and the role of laparoscopic surgery in complicated Meckel's diverticulum in children. We retrospectively reviewed the medical records of 19 patients with complicated Meckel's diverticulum who underwent operation at Asan Medical Center between Jan. 1990 and Apr. 2007. Male to female ratio was 11:8, and median age was 1 year (1 day-13 years). The most frequent symptom was hematochezia (68%), followed by irritability or abdominal pain (16%), vomiting (11%), and abdominal distension (5%). Two operative procedures were performed; small bowel resection with anastomosis (68%) and diverticulectomy (32%). The operation proven complications of the Meckel's diverticulum were bleeding (68%), intussusception (16%), perforation (11%) and obstruction (5%). Ectopic tissues found by postoperative pathologic examination were gastric (84%) and pancreatic (11%). Hospital stay after laparoscopic operation for bleeding Meckel's was 5 days (median) and average first postoperative feeding was 1.5 days. On the contrary, hospital stay for open surgery was 7 days and first feed was 3 days. In summary, the most common compliation of Meckel's diverticulum in children was bleeding and ectopic gastric tissues were present in 84%. Laparoscopic procedure seemed to be useful for diagnosis as well as for definitive treatment.
Citations
We reviewed the records of 25 patients who were re-operated upon after primary repair of esophageal atresia with or without fistula at the Department of Pediatric Surgery, Seoul National University Children's Hospital, from January 1997 to March 2007. Types of the esophageal atresia anomalies were Gross type A in 5 patients, C in 18, and E in 2. The indications for re-operation were anastomosis stricture (n = 14), tracheo-bronchial remnant (n = 4), persistent anastomosis leakage (n = 3), recurrent tracheo-esophageal fistula (n = 2) and esophageal web (n = 2). The interval between primary and secondary surgery was from 48 days to 26 years 5 months (mean: 2 years and 4 months). Four patients required a third operation. The interval between the second and third operation was between 1 year 1 month and 3 year 10 month (mean: 2 years 5 months). Mean follow up period after last operation was 35 months (1 years–8 years 6 months). The secondary surgery was end-to-end esophageal anastomosis in 15, esophagoplasty in 5, gastric tube replacement in 5. After secondary operation, 6 patients had anastomosis stricture (4 patients were relieved of the symptoms by balloon dilatation, 2 patients underwent tertiary operation). Five patients had leakage (sealed on conservative management in all). Two patients had recurrent tracheo-esophagel fistula (1 patient received chemical cauterization and 1 patient underwent tertiary operation). Currently, only one patient has feeding problems. There were no mortalities. Secondary esophageal surgery after primary surgery for esophageal atresia was effective and safe, should be positively considered when complications do not respond to nonoperative therapy.
The use of subcutaneously tunneled, cuffed central venous catheters like Broviac's or Hickman's has increased and complications related to catheter removal has also increased. However, there are only few reports of complications that occur at the time of removal. The authors report an unusual case of catheter fracture during removal of Broviac catheter.
Tapering enteroplasty was first described by Thomas in 1969 as one method of intestinal anastomosis. The advantages of tapering enteroplasty in the intestinal atresia are: First, it makes end-to-end anastomosis possible between the atretic bowel ends with considerable differences in diameters. Second, it promotes the recover of the postoperative bowel function. Third, it prevents the possibility of the short bowel syndrome by eliminating the need of resecting the dilated bowel. A total of 22 patients with intestinal atresia who underwent tapering enteroplasty from January 1988 to December 2005 at our institute were reviewed. In 3 of 22 cases, tapering enteroplasty was the 2nd operation after an initial end-to-oblique anastomosis. We reviewed the following items: age, sex, type and location of intestinal atresia, initial feeding and total enteral feeding start day, the length of hospital stay and complications. The average age of the patients was 7 days. Male to female ratio was 1 to 1.2 (10 cases: 12 cases). We performed the tapering enteroplasty on all types and locations of the intestinal atresia from the duodenum to the colon: type I (n=3), type II (n=4), type IIIA (n=7), type IIIB (n=5), type IIIB and IV (n=1), type IV (n=1) and type C (duodenum) and type IIIB and IV (jejunum). On the average, the oral feeds were started on the postoperative 8.8th day, and full caloric intake via the enteric route was achieved on postoperative 13.3th day. The average length of hospital stay was 19.6 days. There were 1 case (4.5 %) of anastomotic complication and 2 cases (9 %) of adhesive ileus among 22 patients. The tapering enteroplasty on all types of intestinal atresia is a usefull operative method when there are considerable diameter differences between the atretic bowel ends.
Citations
Fundoplication is accepted as an effective treatment of gastroesophageal reflux disease. The recent results of laparoscopic fundoplication demonstrated safety and less morbidity, shorter hospital stay and less pulmonary complication compared to the open operation. Laparoscopic fundoplication has been our first choice of operation for gastroesophageal reflux disease since 2003. Among 29 cases, there were 2 conversion cases because of severe distension of transverse colon and hepatomegaly. We studied 27 consecutive patients operated upon from January 2003 through December 2004. There were 15 boys and 12 girls, ages from 1.5 months to 12 years (median 25.3 months). Body weight ranged from 2.9 kg to 37 kg (median 9.8 kg). Neurological abnormalities were present in 23 patients. Indications for surgery included medically refractory reflux associated with vomiting, pneumopathy, otorhinolaryngologic pathology, failure to thrive, esophagitis, apnea and bradycardia. We used 4-5 trocars of 5 mm or 12 mm with 30° telescope and performed the Nissen technique in all patients. In neurological impaired patients, gastrostomy tube was placed at the time of fundoplication. Median operative time was 130 minutes (70 - 300 minutes). There was no mortality nor intraoperative complication. Twenty-six patients were followed for median of 19 months (8 - 31 months). Four patients (15.4 %), who were all neurological impaired, developed recurrent symptoms of gastroesophageal reflux disease. Two of these patients had reoperation (1 laparoscopic approach, 1 open method). There were significant increases in body weight in 11 patients after fundoplication. Laparoscopic fundoplication is acceptable as a safe and effective method for gastroesophageal reflux disease.
Citations
A one day old female infant was brought to the emergency room suffering from shortness of breath. An x-ray revealed the gastrointestinal tract in the right thoracic cavity. An emergency operation demonstrated eventration of the diaphragm, and a plication was performed. The baby was discharged without complication and has been followed up in the out patient clinic. Congenital diaphragmatic eventuation requiring emergency operation is rare.
Intestinal duplication is a rare congenital anomaly. The diagnostic approach is difficult because of the differences in its location and clinical presentation. To evaluate the diagnostic as well as the therapeutic approaches in children, the medical records of 20 patients with intestinal duplications which had been operated upon from July 1980 to October 2002 were analyzed, retrospectively. The range of age was from 1 day to 11 years. The variables, such as age, sex, clinical presentation, diagnostic method, localization, anatomic type, treatment, complication, and combined anomalies were analyzed. Most of the cases were presented as incidental finding. The majority of the duplications except hindgut were cystic type. Treatment included segmental intestinal resection, excision of the lesion without intestinal resection, and septotomy. Seventy-five percent of the patients were detected before 1 year of age. The anatomic type of the lesion was closely related with its location. The cases of hindgut were almost always tubular type except 1 case. Clinical presentation was related to age, location, and anatomic type. There were no specific diagnostic methods. Perfect localization and application of appropriate operation are the most important requirements for successful treatment.
Citations
A total of 30 cases of the peptic ulcer in children, who underwent operations from January 1981 to December 1995 because of complications at Department of the Surgery, Chonbuk National University Medical School, is reviewed. Twenty-three were males (76.7%), 7 females (23.3%) and male was preponderant at 3.3:1. There were 25 cases (83.3%) age 10 to 15 years, 3 (10.0%) between 2 and 9 years, and 2 (6.7%) below 2. The ulcer was located at duodenum in 27 (90.0%), and at stomach in 3 cases (10.0%). Complications were perforation in 19 cases (63.3%), pyloric obstruction in 9 (30.0%) and bleeding in 2 (6.7%). For perforation, truncal vagotomy with pyloroplasty was done in 11 cases, truncal vagotomy with hemigastrectomy and gastrojejunostomy in 6, and simple closure in 2 cases. For obstruction, truncal vagotomy with hemigastrectomy and gastrojejunostomy was done in 5, and truncal vagotomy and pyloroplasty in 3 cases. For bleeding lesions, truncal vagotomy and pyloroplasty was performed in 2 cases. Ten postoperative complications developed in 9 patients; adhesive ileus in 5, recurrence in 2, pneumonia 2, and wound seroma 1 case. One patient developed a primary duodenal perforation and another a recurrent obstruction. Both of patients had symptoms for more than 3 years and were treated with truncal vagotomy and pyloroplasty for the primary operations. Hospital stay was 11.5 days for the patient with perforated ulcer, 11.0 days for the patient with pyloric obstruction, and 14.5 days for the child with bleeding. Average hospital period was 11.6 days. To reduce recurrences after operation, extensive procedure such as distal gastrectomy with vagotomy at the first operation should be considered in case with severe complication or with patients who have been symptomatic for long periods.
Continuous Ambulatory Peritoneal Dialysis (CAPD) has now become an established form of renal replacement therapy in children. Despite of technical improvements, there are various complications in CAPD. We reviewed medical records of children who received CAPD at Seoul National University Children's Hospital in the period between May 1991 and June 2002. Ninety-three procedures of CAPD catheter insertion in 70 patients were included in this study. Complication rate was 64.5%, and CAPD catheter related peritonitis was most common. In conclusion, CAPD catheter related peritonitis develops in considerable number of pediatric patients. Although the peritonitis could be treated with empirical antibiotics therapy, further investigation to prevent complication is required.
Citations
Anal canal duplications occurring in a pair of 4 month-old healthy female twins are presented. The openings were located in the posterior midline of the anus since birth without a history of perianal abscess or swelling. Excision of the duplicated anal canals was performed using posterior sagittal approach. Although the anal canal duplication occurs predominantly in female, to our knowledge, this is the first case of anal duplication in a monozygotic female twins reported.
This is a 20 year analysis of the problems associated with enterostomy formation, and closure. Forty-three stomas were established in 43 patients: 23 for anorectal malformations, 11 for Hirschsprung's diseases, 4 for necrotizing enterocolitis, 3 for multiple ileal atresias, 1 for volvulus neonatorum with perforation, and 1 for diaphragmatic hernia with colon perforation. Thirty boys and 13 girls were included (mean age 4.8 months). Stoma complications were encountered in 13 patients (30.2 %): stomal prolapse, stenosis, obstruction, paracolic hernia, retraction, dysfunction, and skin excoriation. Four patients (9.3 %) required stomal revision. Occurrence of complications was not related to age and primary disease, but sigmoid colostomy showed lower complication rate than transverse colostomy (20.0 % vs 42.9 %, p<0.05). There were five deaths but, only one (2.3 %) was directly related to the enterostomy complication. Twenty-one stomas were closed in our hospital and complications occurred in seven patients (33.3 %). The most common complication was wound sepsis in 5 children. In conclusion, because the significant morbidity of stomal formation still exists, refinements of the surgical technique seem to be required. Sigmoid loop colostomy is preferred whenever possible.
Citations
Gastrointestinal duplications are rare congenital malformation that may require surgical intervention in the neonate, infant, and occasionally the older child. Symptoms produced by duplications vary according to their location, size, type and histology. We report the clinical characteristics and the surgical results of 9 cases of the gastrointestinal duplications treated at at Asan Medical Center between 1989 and 2000. Five patients were boys and four were girls; age of patients ranged from 5 days to 10 years. Eight duplications were cystic and one was tubular. One involved the stomach; five were in the ileum, and two in the cecum. The most common presentation was intestinal obstruction. There was associated anomaly in one patient, pulmonary sequestration and double ureter. Ectopic gastric mucosa was found in two. All patients underwent surgical resection. There was no perioperative mortality or morbidity. Although gastrointestinal duplication is a rare entity, consideration of associated anomalies and being familiar with the anatomy and clinical features are required for adequate management. In cystic form, complete excision is recommended but planned surgery is required for long segment tubular lesion.
Citations
Eleven children with gastroesophageal reflux disease underwent fundoplication. Eight had neurological impairment, two hiatal hernia and one had history of esophageal repair for esophageal atresia. The most common and significant symptom was vomiting (81.8%), followed by recurrent respiratory infections (72.7%) and failure to thrive (72.7%). The most common diagnostic tool was 24 hour esophageal pH study, which showed a pH less than 4 for more than 10% of the total recorded time in 6 among 9 patients. Nissen fundoplication was performed in 10 patients. Thal fundoplication was carried out in one patient with esophageal atresia. Stamm gastrostomy was added for nutritional and/or swallowing problem in all 8 patients with neurological impairment. The median follow up period was 13 months. There were one late death of unrelated cause and one recurrence. The quality of life after antireflux surgery was greatly improved. Antireflux surgery should be done if indicated, and a simultaneous gastrostomy be considered in a patient with neurological impairment.
Segmental dilatation of small intestine is a rare form of the congenital intestinal anomaly. Many other congenital anomalies have been reported in these patients, but to our knowledge, the association with colonic duplication has not been reported in literatures. We report a case of segmental dilatation of distal ileum associated with colonic duplication. The main clinical and pathogenic aspects are discussed, and the literatures were reviewed.
Intramuscular injection(IM) into the gluteal muscles is a common route of medication, but may lead to complications. A retrospective review of 32 patients who required surgical treatment for local complications of buttock injections in children was made at the Taegu Fatima Hospital during a seven-year ninemonth period (March 1990 to December 1997). Local complications included acute inflammation, cellulitis and abscess(71.9 %), and fat necrosis(21.9 %), and injection granuloma(6.2 %). Over the half of injections were on the upper and outer quadrant of the buttock, but the other 43.7 % were in the upper and inner or lower and outer quadrant which are considered unsuitable sites for intramuscular injection. The majority of complications developed within fat tissue (90.6 %) rather than within muscle(9.4 %). Two-thirds of the patients were under 2 years of age, this suggests that it is technically difficult to accurately administer 1M injections in small children because muscle mass is smaller compared to subcutaneous. In addition subcutaneous fat is more susceptible to chemical irritation. Staph. aureus was the predominant organism, isolated in 84.6 % of the patients with abscesses. Treatment consisted of needle aspiration, incision and drainage, curettage, or surgical excision. In conclusion, the major factor that contributes to complications following 1M of the buttock appears to be the inadvertent intrafat rather than of 1M injection. Accurate injection into the muscles based on a knowledge of pelvic anatomy as well as the potential complications is necessary to prevent complications.
Citations
Reduction of intussusception using air or oxygen has wide acceptance as an alternative to conventional hydrostatic reduction. This study was undertaken to evaluate the results and complications of air pressure enema in 948 pediatric inc tussusception. One hundred and twenty nine cases were operated on at the Department of Surgery, Masan Samsung Hospital from 1985 to 1996 because of air reduction failure. The success rate was 86.4 %. Twenty-one patients(2.2 %) showed perforation during air reduction. Risk prone factors of perforation were; age less than 3 months(42.9 % vs 11.1 %), duration of symptoms greater than 48 hours(66.7 % vs 33.3 %), and presence of pathologic leading point(28.6 % vs 3.7 %). Vomitting and spontaneous rectal bleeding revealed higher prediction to the complication. In ninteen cases, bowel infarction, coagulated necrosis and hemorrhage suggested that the cause of perforation was due to the preexisting strangulation. In conclusion, when doing an air pressure enema reduction, care must be taken if the patient is of a young age or the symptoms are of long duration.
Congenital duplication of the gallbladder, including true duplication and septated gallbladder, is an uncommon but potentially complicated malformation. It presents biliary colic associated with acute or chronic cholecystitis. It can be diagnosed preoperatively by various imaging tools such as real-time ultrasonography, biliary scintigraphy, oral cholecystography, or endoscopic retrograde cholangiography. It can be safely managed by either laparoscopic or open procedures. This report describes a 6-year-old girl with true duplication of gallbladder diagnosed preoperatively by real-time ultrasonography and treated by open cholecystectomy.
Diphallus is a rare congenital anomaly and is frequently associated with duplication of the urinary tract and rectosigmoid, and commonly associated with vertebral anomalies. Remzi reported less than 100 cases of duplication of all or a portion of the penis, but about 10 cases of complete diphallus with exstrophy of cloaca was reported, and a case of complete diphallus associated with hingut duplication was reported, and complete diphallus with displacement of bladder associated hindgut duplication and imperforate anus was not reported in Korea. We experienced a case of the complete diphallus associated with displacement of bladder, hindgut duplication, and imperforate anus as a variant of cloacal exstrophy. A review of published cases suggests that this may be the first example of a complete dip hall us with displacement of bladder coexisting with the hindgut duplication and imperforate anus.
The incidence of Meckel's diverticulum(MD) in general population has been assessed as 2 percent. The major complications of MD are bleeding, perforation, and intestinal obstruction. In spite that the complication rate of Meckel's diverticulum is relatively high(about 4.2% during a lifetime), the preoperative diagnostic rate of complicated MD is very low. Authors investigated the clinical characteristics of complicated MD to improve the diagnostic rate. 16 patients with complicated Meckel's diverticulum who were operated upon at the Department of Pediatric Surgery, Seoul National University Children's Hospital from June 1985 to December 1993 were reviewed. Among the 16 patients with complicated MD, 12 patients(75%) were under 2 year-old and male were predominant(88%). The most common complication was bleeding patients with bleeding MD (8 cases) were diagnosed preoperatively as MD. 8 patients with other complications(perforation : 4 cases, obstruction: 4 cases) could not be suspected as complicated MD except one patient who had previous history of melena. These patients were diagnosed after exploratory laparotomy under the various impression other than MD. Among 12 patients with ulcer related complications such as bleeding and perforation, heterotopic gastric mucosa was found in 11 patients. In conclusion, in any children with unexplained acute abdomen, especially under 2 years old, complicated MD must be included in differential diagnosis. In children with obscure lower gastrointestinal bleeding,99m Tc-pertechnetate scintigraphy is a useful diagnostic tool to rule out bleeding MD.
Citations
 First
First Prev
Prev

