Purpose At our institution, congenital duodenal atresia is repaired laparoscopically using duodenoduodenostomy with a parallel anastomosis. During our use of this technique, we noted that after mobilization, the distal duodenal segment naturally rested in either a cranial or caudal orientation relative to the proximal segment and that this resting orientation appeared to vary with the anatomical level of atresia. This study primarily evaluated the association between atresia location and the natural orientation of the distal duodenal segment. It secondarily compared perioperative outcomes between the cranial and caudal orientation groups.
Methods This retrospective cohort study was conducted at Samsung Medical Center (Seoul, South Korea) and included neonates who underwent laparoscopic duodenoduodenostomy with parallel anastomosis for congenital duodenal atresia from January 2008 to June 2021. After patients with annular pancreas or duodenal web were excluded, 22 neonates were analyzed and categorized into the cranial (n=16) or caudal (n=6) orientation group according to intraoperative findings. Perioperative outcomes were compared, and the relationship between atresia location and distal segment orientation was analyzed.
Results Operative time, postoperative ventilator support, time to feeding initiation, time to full feeding, and length of hospitalization did not differ significantly between groups. No patient required conversion to open surgery, developed an anastomotic stricture, or died during hospitalization. One patient in the cranial group developed an anastomotic leak, which was treated by laparoscopic reanastomosis. First-portion duodenal atresia was significantly more frequent in the caudal group than in the cranial group (83.3% vs. 25.0%, P=0.023).
Conclusion Laparoscopic duodenoduodenostomy with parallel anastomosis was feasible in both cranial and caudal orientations, with no conversions to open surgery. The natural orientation of the distal duodenal segment was significantly associated with the anatomical location of atresia, supporting an anatomical basis for orientation-guided parallel anastomosis.
Purpose This study aimed to compare perioperative outcomes between laparoscopic-assisted diverticulectomy and laparoscopic-assisted small bowel resection for Meckel diverticulum.
Methods This single-center retrospective comparative cohort study included 39 patients who underwent laparoscopic-assisted surgery for Meckel diverticulum at Samsung Medical Center, Korea, between June 2010 and December 2023. Patients were classified into the laparoscopic-assisted diverticulectomy group or the laparoscopic-assisted small bowel resection group. Baseline characteristics, preoperative presentation, operative time, time to first oral feeding, postoperative hospital stay, complications, reoperation, and follow-up outcomes were compared between groups.
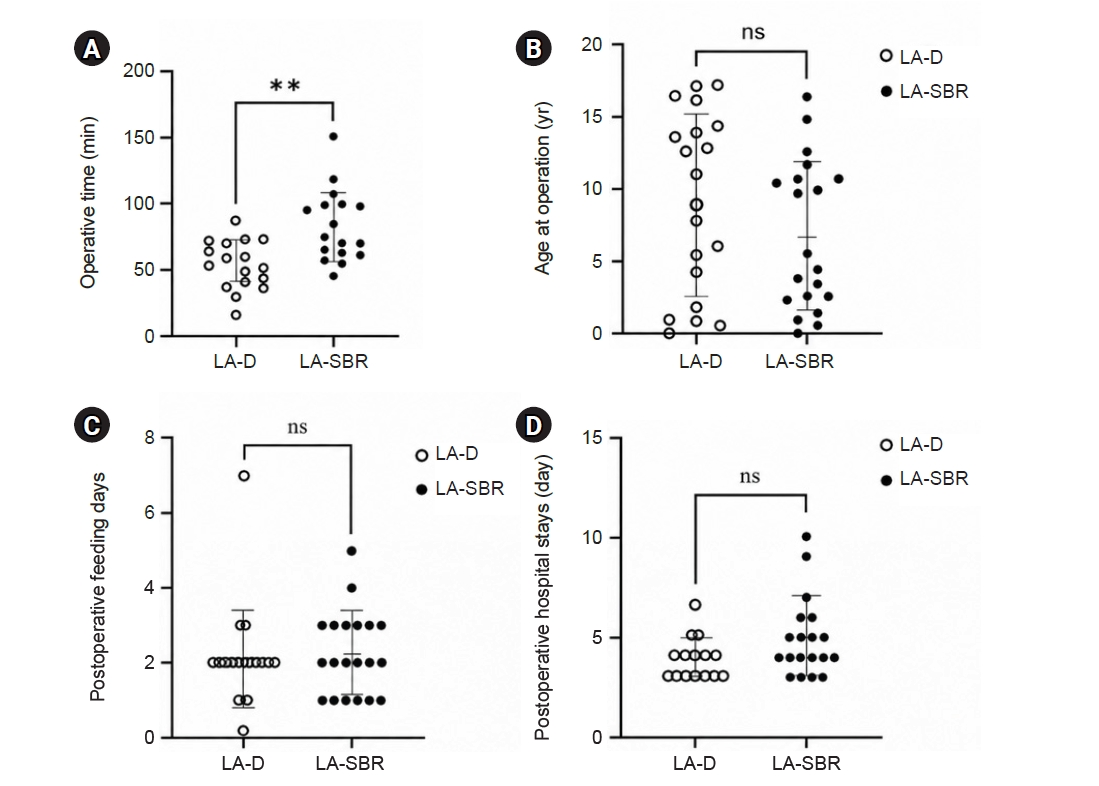
Results Of the 39 patients, 19 underwent laparoscopic-assisted diverticulectomy and 20 underwent laparoscopic-assisted small bowel resection. Baseline characteristics and preoperative presentation did not differ significantly between groups. Operative time was significantly shorter in the diverticulectomy group than in the small bowel resection group (median, 55.0 vs. 76.0 minutes; P=0.002). Time to first oral feeding did not differ significantly between groups (median, 2 days [2–2 days] vs. 2 days [1–3 days]; P=0.397). Postoperative hospital stays also did not differ significantly between groups (median, 4 days [3–4 days] vs. 4 days [4–5 days]; P=0.118), although hospitalization tended to be longer in the laparoscopic-assisted small bowel resection group. No statistically significant difference in complication rates was observed between groups; however, the number of events was low, limiting definitive comparison.
Conclusion Laparoscopic-assisted diverticulectomy was associated with shorter operative time and a tendency toward shorter postoperative hospital stay than small bowel resection, without an observed increase in early complications. It may be a reasonable option for carefully selected patients with uncomplicated Meckel diverticulum.
Jinyoung Park, Dayoung Ko, Hyunhee Kwon, Dae Yeon Kim, Seong Chul Kim, Soo-Hong Kim, Wontae Kim, Hyun-Young Kim, So Hyun Nam, Jung-Man Namgoong, Sungjoo Park, Junbeom Park, Min-Jung Bang, Jeong-Meen Seo, Ji-Young Sul, Joohyun Sim, Soo Min Ahn, Hee-Beom Yang, Jung-Tak Oh, Chaeyoun Oh, Joong Kee Youn, Sanghoon Lee, Ju Yeon Lee, Cheolgu Lee, Kyong Ihn, Soo-Min Jung, Yeon Jun Jeong, Eunyoung Jung, Jae Hee Chung, Min Jeng Cho, Suhyeon Ha, Seok Joo Han, In Geol Ho
Adv Pediatr Surg 2026;32(1):18-26. Published online June 22, 2026
Purpose This study investigated the clinical characteristics, anatomical distribution, operative management, and postoperative outcomes of pediatric patients who underwent surgery for intestinal duplication and were registered through a nationwide multicenter survey conducted by the Korean Association of Pediatric Surgeons (KAPS).
Methods KAPS conducted a nationwide multicenter retrospective survey across 18 institutions between 2020 and 2024 and collected data from 144 patients.
Results Female patients accounted for 55.6% of surgically treated cases, corresponding to a male to female ratio of 1:1.25. Vomiting and abdominal pain were the most common presenting symptoms. Prenatal diagnosis was achieved in 43.7% of cases. The ileum was the most common site of intestinal duplication (41.0%). Cystic duplications predominated (82.6%), and communication with the native bowel was documented in 19.4% of cases. Elective surgery was performed in 83.3% of patients, with laparoscopic-assisted surgery being the most commonly used approach (52.8%). The most frequently performed surgical procedures were excision (49.3%) and bowel resection with anastomosis (47.2%). Recurrence occurred in three patients (2.1%), and mortality was reported in one patient (0.7%).
Conclusion This study represents the largest multicenter dataset on intestinal duplication in South Korea and provides comprehensive information regarding its clinical characteristics and surgical outcomes. These findings may serve as a useful reference for understanding the clinical spectrum and operative management of pediatric intestinal duplication in South Korea and may support the development of future standardized prospective studies.
Yeon Jun Jeong, Dayoung Ko, Hyunhee Kwon, Ki Hoon Kim, Dae Yeon Kim, Soo-Hong Kim, Wontae Kim, Hae-Young Kim, Hyun Young Kim, Seong Chul Kim, Younghyun Na, Jung-Man Namgoong, So Hyun Nam, Junbeom Park, Jinyoung Park, Tae-Jun Park, Jeong-Meen Seo, Ji-Young Sul, Joonhyuk Son, Hyun Beak Shin, Joohyun Sim, Soo Min Ahn, Hee Beom Yang, Jung-Tak Oh, Chaeyoun Oh, Joong Kee Youn, Sanghoon Lee, Ju Yeon Lee, Kyong Ihn, Hye Kyung Chang, Eunyoung Jung, Jae Hee Chung, Yu Jeong Cho, Yun Mee Choe, Soo Jin Na Choi, Seok Joo Han, In Geol Ho, Ji-Won Han
Adv Pediatr Surg 2025;31(2):47-58. Published online July 16, 2025
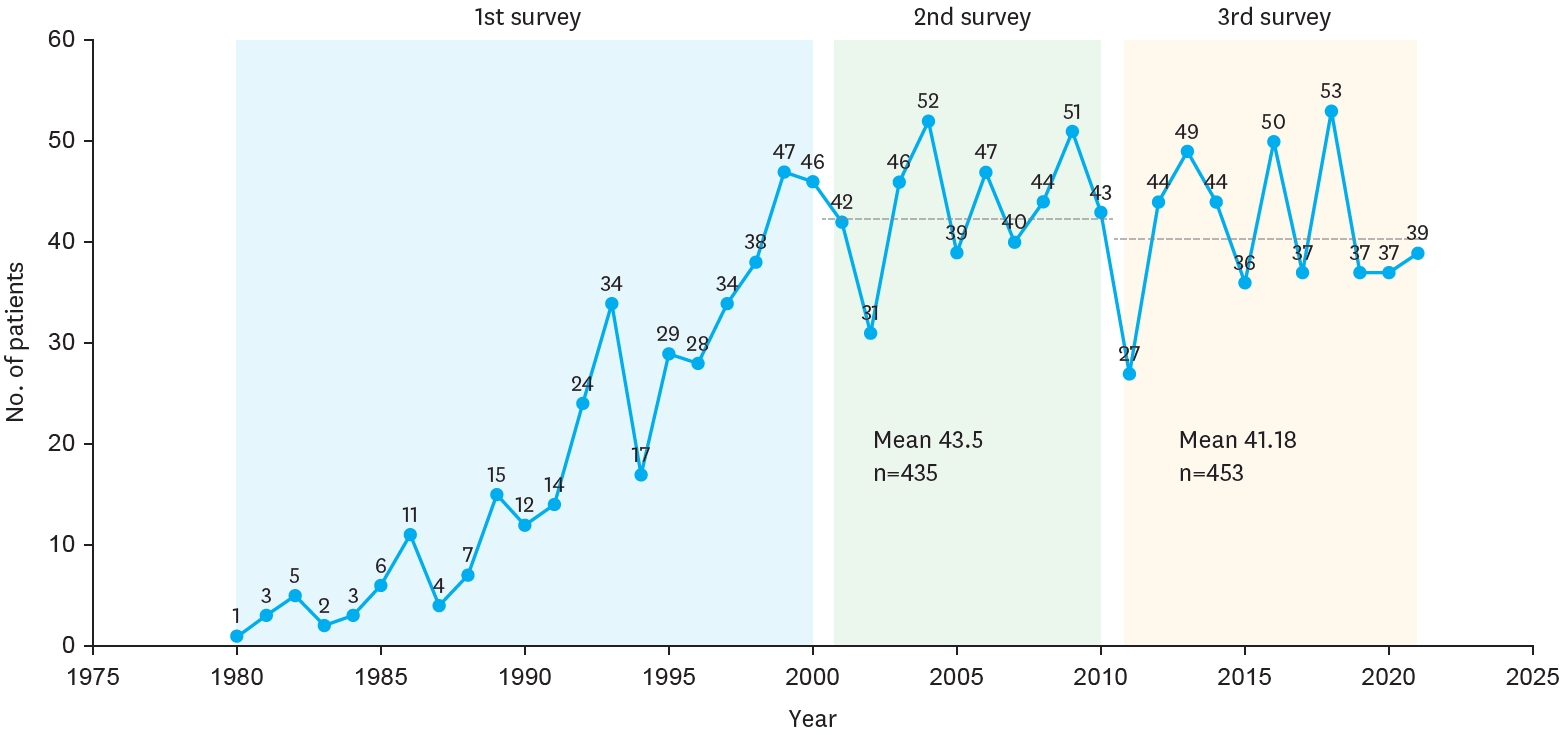
Purpose Biliary atresia (BA) is a rare but progressive cholangiopathy and the leading cause of pediatric liver transplantation worldwide. The Korean Association of Pediatric Surgeons (KAPS) has conducted three national surveys (2001, 2011, and 2023) to assess long-term trends in the diagnosis, treatment, and outcomes of BA. This study provides a comparative analysis of the 2nd and 3rd national surveys, with reference to selected findings from the 1st survey.
Methods This study included 453 patients from the 3rd national survey (2011–2021) and 435 patients from the 2nd survey (2001–2010), all of whom underwent Kasai portoenterostomy. Data were collected via electronic case report forms from pediatric surgical centers nationwide. Comparisons were made regarding demographics, clinical features, diagnostic patterns, operative details, follow-up outcomes, and survival. Kaplan–Meier analysis was used to evaluate long-term survival.
Results The mean number of BA patients per year remained stable between surveys (43.5 in the 2nd, 41.18 in the 3rd), though centralization of care increased, with 61.5% of cases managed by two major institutions in the 3rd survey. The median age at surgery decreased, and the use of preoperative imaging (especially magnetic resonance cholangiopancreatography) increased. The 10-year native liver survival rate declined from 59.8% to 53.7%, while overall 10-year survival improved slightly (92.9% to 93.2%). Postoperative complications, such as cholangitis and liver failure, persisted but were better categorized. The 3rd survey also reported improved mortality (4.9%) and reduced follow-up loss (11.5%) compared to the 2nd survey.
Conclusion While overall survival after Kasai operation has remained high and even improved, native liver survival has slightly declined. The findings reflect earlier diagnosis, more consistent diagnostic imaging, and increasing centralization of care. These trends underscore the importance of long-term nationwide data collection in guiding future strategies for BA management in Korea.
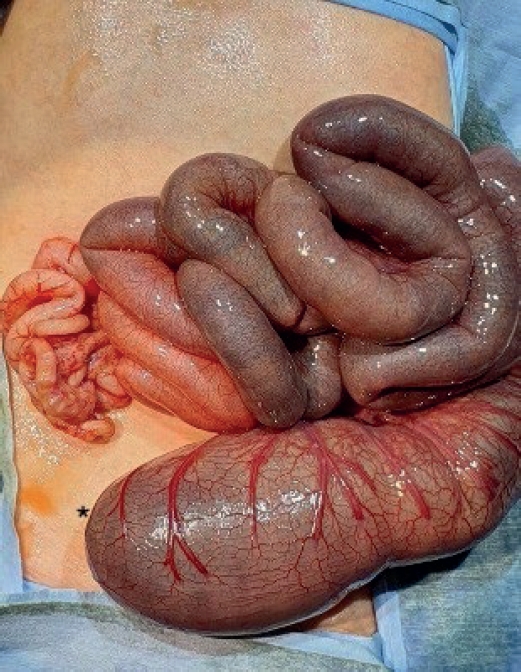
The concurrent occurrence of colonic atresia, malrotation, and Hirschsprung’s disease in neonates is extremely rare. These anomalies often share embryologic origins and present overlapping clinical symptoms that complicate diagnosis and management. We report two neonatal cases with this rare triad. Case 1 involved a term neonate initially diagnosed with esophageal atresia and later found to have colonic atresia, malrotation, and Hirschsprung’s disease. Case 2 was a preterm neonate presenting with abdominal distension and perforation, ultimately diagnosed with the same triad. Both underwent staged surgical management, including Duhamel’s procedures after confirming aganglionosis. Awareness of the possible coexistence of these anomalies is essential in neonates with colonic atresia and non-fixed colon. Surgical planning should anticipate aganglionosis and include rectal biopsy. This report emphasizes the importance of early suspicion and multidisciplinary approach for optimal outcomes.
Jinyoung Park, Dayoung Ko, Eun-jung Koo, Hyunhee Kwon, Ki Hoon Kim, Dae Yeon Kim, Seong Chul Kim, Soo-Hong Kim, Wontae Kim, HaeYoung Kim, Hyun-Young Kim, So Hyun Nam, Jung-Man Namgoong, Junbeom Park, Taejin Park, Min-Jung Bang, Jeong-Meen Seo, Ji-Young Sul, Joonhyuk Son, Joohyun Sim, Soo Min Ahn, Hee-Beom Yang, Jung-Tak Oh, Chaeyoun Oh, Joong Kee Youn, Sanghoon Lee, Ju Yeon Lee, Kyong Ihn, Hye Kyung Chang, Yeon Jun Jeong, Eunyoung Jung, Jae Hee Chung, Min Jeong Cho, Yun-Mee Choe, Seok Joo Han, In Geol Ho, Jeong Hong
Adv Pediatr Surg 2025;31(1):8-15. Published online May 28, 2025
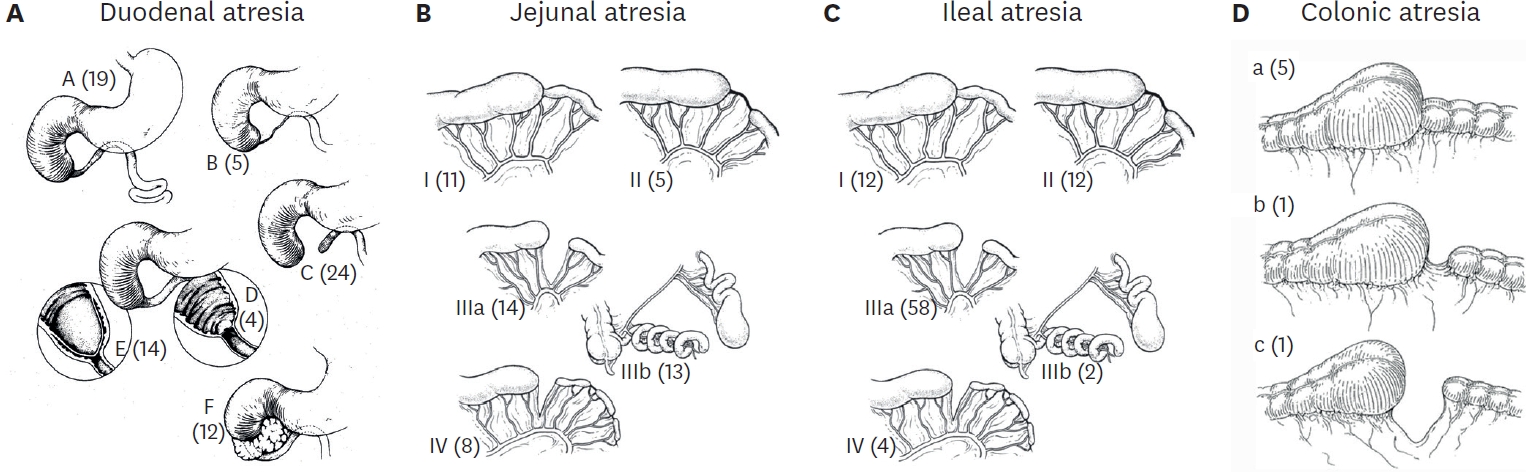
Purpose This study aims to investigate and compare the incidence, demographic characteristics, clinical manifestations, preoperative diagnostic methods, anatomical classifications, associated anomalies, operative treatments, and postoperative outcomes of patients with intestinal atresia treated by the members of the Korean Association of Pediatric Surgeons (KAPS) through three nationwide surveys.
Methods KAPS conducted 3 national surveys in 1998, 2010, and 2024 to examine the patients diagnosed with intestinal atresia. In preparation for the survey, we developed a customized case registration form to obtain data on patient sex, birth weight, gestational age, clinical manifestations, preoperative diagnostic methods, anatomical types, associated anomalies, operative treatments, and postoperative outcomes. Authorized KAPS members completed the case registration form.
Results The first, second, and third national surveys included 218, 222, and 236 individuals diagnosed with intestinal atresia, respectively. The male-to-female ratios were 1.5:1, 1.1:1, and 1.1:1, respectively. The first, second, and third national surveys revealed that 34.3%, 43.3%, and 53.4% of patients were born before 37 weeks of gestation, respectively. Additionally, 28.7%, 32.0%, and 40.7% of patients had a birth weight under 2,500 g. In the third national survey, duodenoduodenostomy was the most common procedure, performed in 70 out of 82 patients diagnosed with duodenal atresia. Resection and anastomosis were the main surgical procedures conducted in 47 out of 54 cases of jejunal atresia and 74 out of 92 cases of ileal atresia. The mortality rates in the first, second, and third national surveys were 13.8%, 3.6%, and 1.3% respectively, with the lowest rate observed in the third national survey.
Conclusion These national surveys offer valuable insights into the current state of intestinal atresia, including specific surgical interventions and postoperative outcomes in South Korea. For pediatric surgeons aiming to enhance their understanding of intestinal atresia and its treatment options, these surveys could be an indispensable resource and guide.
Purpose This study aimed to evaluate postoperative outpatient follow-up practices among pediatric surgeons in Korea for five common congenital diseases: esophageal atresia with tracheoesophageal fistula (EA/TEF), anorectal malformation (ARM), Hirschsprung’s disease (HSCR), choledochal cyst (CC), and inguinal hernia (IH).
Methods A web-based survey consisting of 43 questions was distributed to members of the Korean Association of Pediatric Surgeons. The survey assessed the timing, frequency, and duration of outpatient follow-up, as well as disease-specific practices.
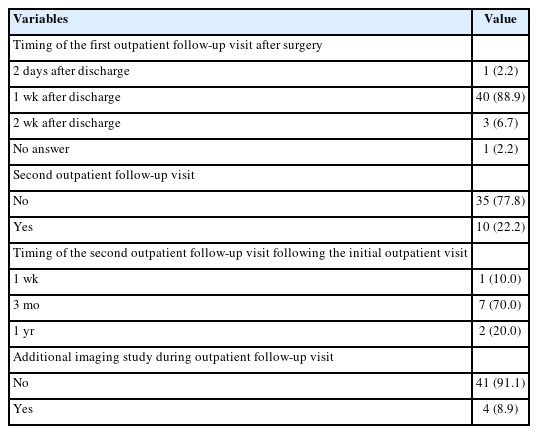
Results Of 154 invited surgeons, 45 (29.2%) responded. Most scheduled the first follow-up visit within one week after discharge. During the first postoperative year, follow-up visits were commonly held every three months, followed by six months or annual intervals. Most surgeons concluded follow-up before age 18; however, 15.6%–37.8% reported continuing follow-up into adulthood depending on the disease. Variation was observed in disease-specific practices: 44.4% routinely performed contrast studies for EA/TEF follow-up; sizes #14–15 Hegar dilators were most used in ARM; only 6.7% performed routine rectal irrigation in HSCR. For CC, 88.9% checked both blood tests and ultrasonography. Most IH patients received only one follow-up visit.
Conclusion While early postoperative follow-up practices among pediatric surgeons in Korea appear relatively consistent, wide variation exists in long-term strategies and disease-specific protocols. This reflects the tendency to rely on individual clinical judgment and highlights the need for standardized, national consensus.
Citations
Citations to this article as recorded by
Transition of Care to Late Adolescent/Adults in Paediatric Surgery: Perspectives From Indian Paediatric Surgeons Sunita Singh, Yogesh Kumar Sarin, Subhashis Saha, Mukesh Shukla Journal of Indian Association of Pediatric Surgeons.2026; 31(4): 541. CrossRef
Yeon Jun Jeong, Dayoung Ko, Eun-Jung Koo, Hyunhee Kwon, Dae Yeon Kim, Soo-Hong Kim, Wontae Kim, Hae-Young Kim, Hyun Young Kim, Seong Chul Kim, Younghyun Na, Jung-Man Namgoong, So Hyun Nam, Sungjoo Park, Junbeom Park, Jinyoung Park, Tae-Jun Park, Jeong-Meen Seo, Ji-Young Sul, Joonhyuk Son, Hyun Beak Shin, Joohyun Sim, Jung-Tak Oh, Chaeyoun Oh, Joong Kee Youn, Sanghoon Lee, Ju Yeon Lee, Cheolgu Lee, Kyong Ihn, Eunyoung Jung, Jae Hee Chung, Yong-Hoon Cho, Yun Mee Choe, Soo Jin Na Choi, Seok Joo Han, In Geol Ho
Adv Pediatr Surg 2024;30(2):39-51. Published online December 13, 2024
Purpose This study provides insights into the prevalence at birth, clinical characteristics, and outcomes of gastroschisis and omphalocele in Korea over the past decade, addressing the lack of localized data despite advanced healthcare capabilities.
Methods The study retrospectively analyzed data from 20 pediatric surgical centers in Korea from January 2012 to December 2021, including 269 patients diagnosed with gastroschisis or omphalocele. Data variables included gender, gestational age, birth weight, associated anomalies, type of defect, surgical interventions, and outcomes.
Results The study covered 269 patients, with 80 gastroschisis and 189 omphalocele cases. Gastroschisis prevalence at birth remained stable at 2.15 per 100,000 live births, while omphalocele increased to 5.08 per 100,000. Both conditions had similar gender ratios (0.95). Gastroschisis patients had lower birth weights (2,463.90±505.50 g) and smaller head circumferences (31.97±1.86 cm) compared to omphalocele patients (2,757.65±761.24 g, 32.78±2.64 cm). Omphalocele cases had more associated anomalies, especially cardiovascular issues. Prenatal diagnosis rates were high: 93.7% for gastroschisis and 86.4% for omphalocele. About 96.3% of gastroschisis and 84.1% of omphalocele patients were born in their treatment hospitals. Gastroschisis patients underwent surgery sooner (average 3.5 days) and started feeding later (16.5 days) than omphalocele patients (average 56.5 days to surgery, 6.6 days to start feeding). Hospital stays and follow-up durations were similar, averaging around 782.6 days for gastroschisis and 800.3 days for omphalocele patients. Survival rates were 89.7% for gastroschisis and 87.1% for omphalocele.
Conclusion The study highlights the need for early diagnosis, centralized care, and specialized surgical approaches to optimize outcomes for gastroschisis and omphalocele patients in Korea. Enhanced prenatal screening and surgical protocols are recommended to improve these patients' prognosis.


 First
First Prev
Prev

