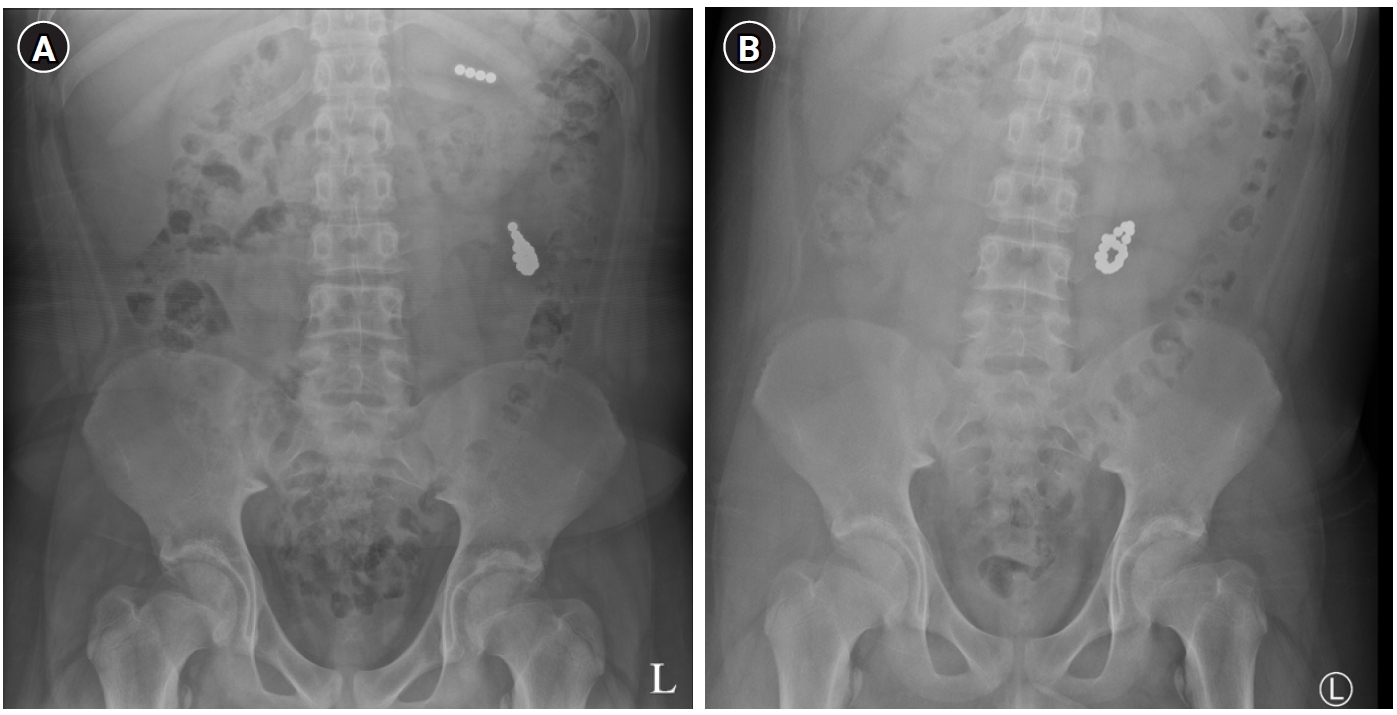
This review summarizes the epidemiology, diagnosis, and management of pediatric foreign body (FB) ingestion, with particular emphasis on circumstances that may require surgical involvement. Initial evaluation includes history taking, assessment of symptoms, and radiographic imaging to determine the type and location of the ingested object. Plain radiography remains the primary diagnostic modality for detecting radiopaque objects and localizing them within the gastrointestinal tract; however, additional imaging may be needed for radiolucent objects or when complications are suspected. Management depends on the anatomical location and characteristics of the FB. Esophageal FBs generally require urgent endoscopic removal, especially when button batteries, magnets, or sharp objects are involved. After an object has passed into the stomach, many cases can be managed conservatively; however, high-risk objects, including button batteries, multiple magnets, and long or sharp items, may require early removal. FBs beyond the pylorus usually pass spontaneously but require monitoring for complications. Surgical intervention may be necessary when endoscopic removal is not feasible or when complications such as obstruction, perforation, or fistula formation occur. This review summarizes location- and object-specific management strategies and identifies situations in which early surgical involvement may improve outcomes in children with FB ingestion.
Purpose Enteric duplication cysts (EDCs) are rare congenital anomalies of the gastrointestinal tract. This study aimed to delineate the clinical, anatomical, and pathological spectrum of EDCs based on a 40-year single-center experience.
Methods A retrospective review was conducted of 45 pediatric patients who underwent surgical treatment for EDCs at a single institution between 1985 and 2023. Clinical records, imaging studies, and pathological reports were analyzed.
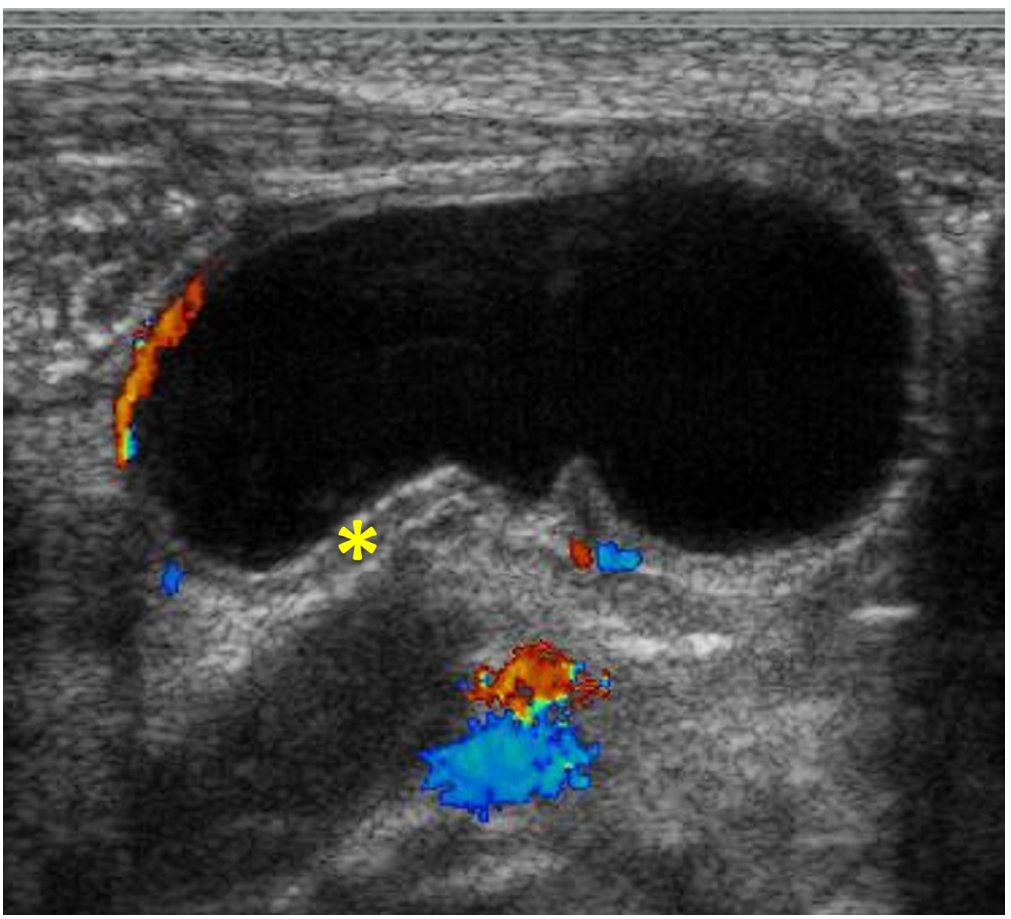
Results The study included 28 males and 17 females, with a median age at surgery of 4.7 months. Most patients (75.6%) underwent surgery before 2 years of age. The ileum was the most common location (57.8%), followed by the jejunum (11.1%) and ileocecal valve (11.1%). Vomiting (46.7%) was the most common presenting symptom. Emergency surgery was required in 28.9% of cases because of complications such as volvulus or intussusception. Preoperative imaging using ultrasonography (US) and/or computed tomography resulted in a correct diagnosis in 34 of 45 patients (75.6%), with EDCs correctly identified in 30 patients (66.7%), frequently based on the characteristic “double wall sign” observed on US. Histopathological examination identified heterotopic gastric mucosa in 61.4% of evaluable cases. Postoperative outcomes were generally favorable, with a median hospital stay of 7.5 days.
Conclusion EDCs are rare congenital anomalies that are primarily diagnosed during early childhood. The ileum is the most frequent site of involvement, and clinical presentation is often related to acute complications. Prompt and complete surgical excision remains the definitive treatment and leads to favorable short-term postoperative outcomes, with no recurrence observed during the available follow-up period.
Jinyoung Park, Dayoung Ko, Hyunhee Kwon, Dae Yeon Kim, Seong Chul Kim, Soo-Hong Kim, Wontae Kim, Hyun-Young Kim, So Hyun Nam, Jung-Man Namgoong, Sungjoo Park, Junbeom Park, Min-Jung Bang, Jeong-Meen Seo, Ji-Young Sul, Joohyun Sim, Soo Min Ahn, Hee-Beom Yang, Jung-Tak Oh, Chaeyoun Oh, Joong Kee Youn, Sanghoon Lee, Ju Yeon Lee, Cheolgu Lee, Kyong Ihn, Soo-Min Jung, Yeon Jun Jeong, Eunyoung Jung, Jae Hee Chung, Min Jeng Cho, Suhyeon Ha, Seok Joo Han, In Geol Ho
Adv Pediatr Surg 2026;32(1):18-26. Published online June 22, 2026
Purpose This study investigated the clinical characteristics, anatomical distribution, operative management, and postoperative outcomes of pediatric patients who underwent surgery for intestinal duplication and were registered through a nationwide multicenter survey conducted by the Korean Association of Pediatric Surgeons (KAPS).
Methods KAPS conducted a nationwide multicenter retrospective survey across 18 institutions between 2020 and 2024 and collected data from 144 patients.
Results Female patients accounted for 55.6% of surgically treated cases, corresponding to a male to female ratio of 1:1.25. Vomiting and abdominal pain were the most common presenting symptoms. Prenatal diagnosis was achieved in 43.7% of cases. The ileum was the most common site of intestinal duplication (41.0%). Cystic duplications predominated (82.6%), and communication with the native bowel was documented in 19.4% of cases. Elective surgery was performed in 83.3% of patients, with laparoscopic-assisted surgery being the most commonly used approach (52.8%). The most frequently performed surgical procedures were excision (49.3%) and bowel resection with anastomosis (47.2%). Recurrence occurred in three patients (2.1%), and mortality was reported in one patient (0.7%).
Conclusion This study represents the largest multicenter dataset on intestinal duplication in South Korea and provides comprehensive information regarding its clinical characteristics and surgical outcomes. These findings may serve as a useful reference for understanding the clinical spectrum and operative management of pediatric intestinal duplication in South Korea and may support the development of future standardized prospective studies.
Purpose This study aimed to compare perioperative outcomes between laparoscopic-assisted diverticulectomy and laparoscopic-assisted small bowel resection for Meckel diverticulum.
Methods This single-center retrospective comparative cohort study included 39 patients who underwent laparoscopic-assisted surgery for Meckel diverticulum at Samsung Medical Center, Korea, between June 2010 and December 2023. Patients were classified into the laparoscopic-assisted diverticulectomy group or the laparoscopic-assisted small bowel resection group. Baseline characteristics, preoperative presentation, operative time, time to first oral feeding, postoperative hospital stay, complications, reoperation, and follow-up outcomes were compared between groups.
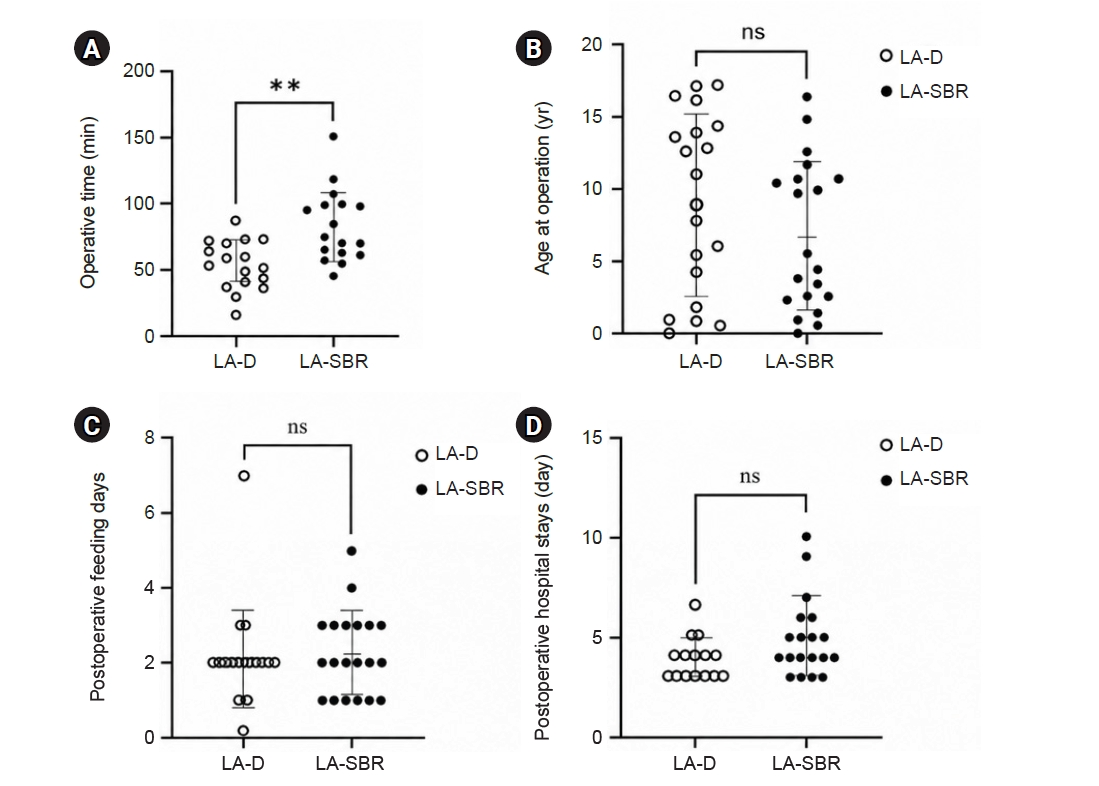
Results Of the 39 patients, 19 underwent laparoscopic-assisted diverticulectomy and 20 underwent laparoscopic-assisted small bowel resection. Baseline characteristics and preoperative presentation did not differ significantly between groups. Operative time was significantly shorter in the diverticulectomy group than in the small bowel resection group (median, 55.0 vs. 76.0 minutes; P=0.002). Time to first oral feeding did not differ significantly between groups (median, 2 days [2–2 days] vs. 2 days [1–3 days]; P=0.397). Postoperative hospital stays also did not differ significantly between groups (median, 4 days [3–4 days] vs. 4 days [4–5 days]; P=0.118), although hospitalization tended to be longer in the laparoscopic-assisted small bowel resection group. No statistically significant difference in complication rates was observed between groups; however, the number of events was low, limiting definitive comparison.
Conclusion Laparoscopic-assisted diverticulectomy was associated with shorter operative time and a tendency toward shorter postoperative hospital stay than small bowel resection, without an observed increase in early complications. It may be a reasonable option for carefully selected patients with uncomplicated Meckel diverticulum.
Purpose At our institution, congenital duodenal atresia is repaired laparoscopically using duodenoduodenostomy with a parallel anastomosis. During our use of this technique, we noted that after mobilization, the distal duodenal segment naturally rested in either a cranial or caudal orientation relative to the proximal segment and that this resting orientation appeared to vary with the anatomical level of atresia. This study primarily evaluated the association between atresia location and the natural orientation of the distal duodenal segment. It secondarily compared perioperative outcomes between the cranial and caudal orientation groups.
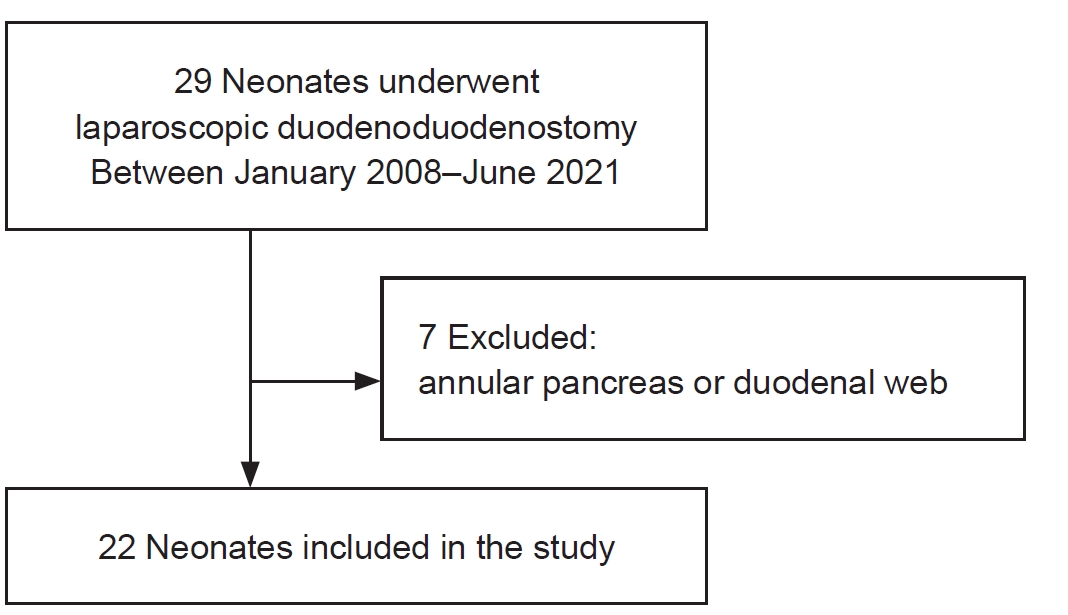
Methods This retrospective cohort study was conducted at Samsung Medical Center (Seoul, South Korea) and included neonates who underwent laparoscopic duodenoduodenostomy with parallel anastomosis for congenital duodenal atresia from January 2008 to June 2021. After patients with annular pancreas or duodenal web were excluded, 22 neonates were analyzed and categorized into the cranial (n=16) or caudal (n=6) orientation group according to intraoperative findings. Perioperative outcomes were compared, and the relationship between atresia location and distal segment orientation was analyzed.
Results Operative time, postoperative ventilator support, time to feeding initiation, time to full feeding, and length of hospitalization did not differ significantly between groups. No patient required conversion to open surgery, developed an anastomotic stricture, or died during hospitalization. One patient in the cranial group developed an anastomotic leak, which was treated by laparoscopic reanastomosis. First-portion duodenal atresia was significantly more frequent in the caudal group than in the cranial group (83.3% vs. 25.0%, P=0.023).
Conclusion Laparoscopic duodenoduodenostomy with parallel anastomosis was feasible in both cranial and caudal orientations, with no conversions to open surgery. The natural orientation of the distal duodenal segment was significantly associated with the anatomical location of atresia, supporting an anatomical basis for orientation-guided parallel anastomosis.
Benign cystic mesothelioma (BCM) is a rare intra-abdominal tumor and is particularly uncommon in pediatric patients. Its nonspecific clinical and radiological features often make preoperative diagnosis challenging. We report the case of a 4-year-old girl who presented with acute abdominal pain and vomiting. Computed tomography revealed a large, multiloculated cystic mass occupying the lower abdomen, which was initially suspected to be a lymphatic malformation. During laparoscopic exploration, a hemorrhagic, multiloculated cystic mass with hemoperitoneum was identified and completely resected with preservation of the right ovary. Histopathological examination confirmed BCM, showing predominant clusters of epithelioid cells interspersed with cyst-like spaces on hematoxylin and eosin staining. The patient recovered uneventfully and had no recurrence during 30 months of follow-up. This case describes an unusual presentation of BCM as an acute abdomen complicated by hemoperitoneum in a child and emphasizes the importance of surgical exploration and histopathological evaluation in establishing the diagnosis.





 First
First Prev
Prev

