
We evaluated perioperative and long-term outcomes of minimally invasive surgery (MIS) and established indications of MIS in solid pseudopapillary tumor (SPT) in pediatric patients.
From October 1992 to April 2018, 66 patients (age, <18 years) diagnosed with SPT underwent either open pancreatectomy (OP) or MIS. Variables including postoperative complications and recurrence rates were retrospectively analyzed.
Thirty-five patients underwent open surgery and 31 underwent laparoscopic/robotic surgery. Mean tumor size in MIS was significantly smaller than that in OP (4.3±1.8 cm vs. 7.6±3.5 cm, p=0.005). There were 4 cases of open conversion from laparoscopic surgery because of vessel encasements (n=2), bleeding (n=1), and pancreatic ductal injury (n=1). Solitary pseudopapillary carcinoma was diagnosed in 6 patients. Recurrence was observed in 3 and 1 patients who underwent OP and MIS, respectively (p=0.634). Tumor size, mass size/abdominal diameter (MS/AD) ratio, and degree of the portal or superior mesenteric vein involvement were the most important indications for MIS.
MIS is being widely used in pediatric surgeries with increased expertise and safety, especially in pancreatic diseases. Careful patient selection for MIS in regards with parameters such as MS/AD ratio and vessel abutment might be a feasible choice.
Citations
This study aimed to evaluate the relationship between nutritional support and growth velocity after abdominal surgery in neonates.
The electronic medical records of 45 neonates who underwent abdominal surgery in neonatal intensive care unit from 2012 to 2016 were collected to see how surgery and postoperative nutrition affect for the growth of neonate with abdominal surgery. The growth velocity was measured from the time of surgery to the time of discharge based on body weight.
In neonates who achieve their protein requirement on the first day after surgery, the growth velocity was better than that in neonates who did not achieve their protein requirement on the first day after surgery (4.31 vs. 15.21; p=0.004). Based on the type of surgery, length of bowel resection and surgical complications, this study showed better growth velocity in neonates who had no surgical complications (5.34 vs. 12.74; p=0.775), reoperation (5.25 vs. 22.19, p=0.987), or bowel resection (6.79 vs. 9.95, p=0.302). However, there was no statistically significant difference among these factors.
We concluded in this study that adequate protein supplement from the first day of surgery could have a positive effect on the growth velocity of neonates who underwent abdominal surgery.
The single stage transanal pull-through (SSPT) for Hirschsprung’s disease is becoming the most popular procedure. This single center study compared the result of single stage operation with two-stage operation for Hirschsprung’s disease in neonates.
We retrospectively reviewed medical records of all patients who were diagnosed as Hirschsprung’s disease and underwent SSPT or two-stage operation operation in Asan Medical Center between January 2003 and July 2014.
There were 17 SSPT and 28 two-stage operation. The mean age of SSPT group was 14.2±7.1 days, and the mean age of two-stage operation group was 15.4±8.6 days for stomy formation, and 188.6±36.3 days for Duhamel operation. The operation time of SSPT was shorter than Duhamel operation (145.0±37.0 minutes vs. 193.0±36.0 minutes, p<0.001). The mean follow-up period of SSPT and two-stage operation was 35.5±34.9 months (range, 2-132 months) and 56.6±35.5 months (range, 1-121 months), respectively. Defecation problem rate such as fecal soiling or fecal impaction showed no significant difference between the two groups (p=0.719). Two SSPT patients required botulinum toxin injection due to rectal stenosis. Three patients of SSPT group underwent re-do endorectal pull-through due to remnant aganglionic or hypoganglionic bowel.
The SSPT showed shorter hospital days. However, few patients experienced rectal stenosis, but were manageable with botulinum toxin injection. The SSPT requires experienced-pathologist, as well as surgeon, because intra-operation pathology reading is critical for appropriate SSPT. SSPT is a feasible and reasonable option to treat Hirschsprung’s disease.
Citations
The aim of this study was to analyze of the risk factors for surgical procedure on ileo-colic intussusception without leading point in children.
We retrospectively reviewed medical records of patient treated for ileo-colic intussusception between January 2003 and December 2014. We exclude the patients who had leading point. Because of the large difference on patient's numbers between non-operative group (cases of ileo-colic intussusceptions successfully reduced by air reduction) and operative group (cases underwent operation due to failed air reduction), we compared the data of operative group of patients without leading point between 2003 and 2014 with the data of non-operative group as control group from 2013 to 2014. Clinical features such as gender, age, body temperature, body weight in diagnosis, growth curves for age-gender-body weight, and laboratory data of blood test were compared.
In non-operative group, total 94 patients who were treated successfully by the non-operative air reduction. In operative group, total 21 patients treated by surgical procedure. The age under 12 months, weight over upper 75 percentile group, increased segment neutrophil count, decreased hemoglobin level and lymphocyte count were significantly associated with a requirement for surgical procedure.
We conclude that younger age, higher weight percentile group, increased segment neutrophil, decreased hemoglobin and lymphocyte are the independent risk factors related to operative treatment for ileo-colic intussusception in children. If primary air reduction is failed in patients with such risk factors, operative treatment over ultrasonography or secondary reduction can prevent unnecessary effort and complications, thus emphasizing the consideration of operative treatment when selecting treatment methods.
Citations
National survey for newborns surgery with congenital anomalies by Korean Association of Pediatric Surgeons (KAPS) was done. A questionnaire was sent to all members of the KAPS on March 2014. The current survey is to review three years status of the newborn surgery from 2012 to 2013. Thirty-four members (27.9%) took part in the survey that included data for the diagnosis, number and procedures of neonatal surgical cases. The result was discussed at the Topic Discussion section of the 30th Annual Congress of KAPS, 2014.
Citations
Minimal invasive surgery (MIS) has rapidly gained acceptance for the management of a wide variety of pediatric diseases. A questionnaire was sent to all members of the Korean Association of Pediatric Surgeons. Thirty one members (25.4%) took part in the survey that included data for the year 2012: demographic details, opinion regarding minimal invasive surgery and robotic surgery, spectrum of minimally invasive operations, and quantity of procedures. 48.4% of the respondents had more than 10 years experience, 35.5% less than 10 years experience, and 16.1 % had no experience. The respondents of the recommend MIS and perform MIS for surgical procedures are as follow; inguinal hernia (61.3%), simple appendicitis (87.1%), complicated appendicitis (80.6%), reduction of intussusceptions (83.9%), pyloromyotomy (90.3%), fundoplication (96.8%), biopsy and corrective surgery of Hirschsprung's disease (93.5%/90.3%), imperforate anus (77.4%), congenital diaphragmatic hernia (80.6%), and esophageal atresia (74.2%). The MIS procedures with more than 70% were lung resection (100%), cholecystectomy (100%), appendectomy (96.2%), ovarian torsion (86.7%), fundoplication (86.8%), hiatal hernia repair (82.6%), and splenectomy (71.4%). The MIS procedures with less than 30% were congenial diaphragmatic hernia reapir (29.6%), esophageal atresia (26.2%), correction of malroatation (24.4%), inguinal hernia repair (11.4%), anorectal malformation (6.8%), Kasai operation (3.6%).
Citations
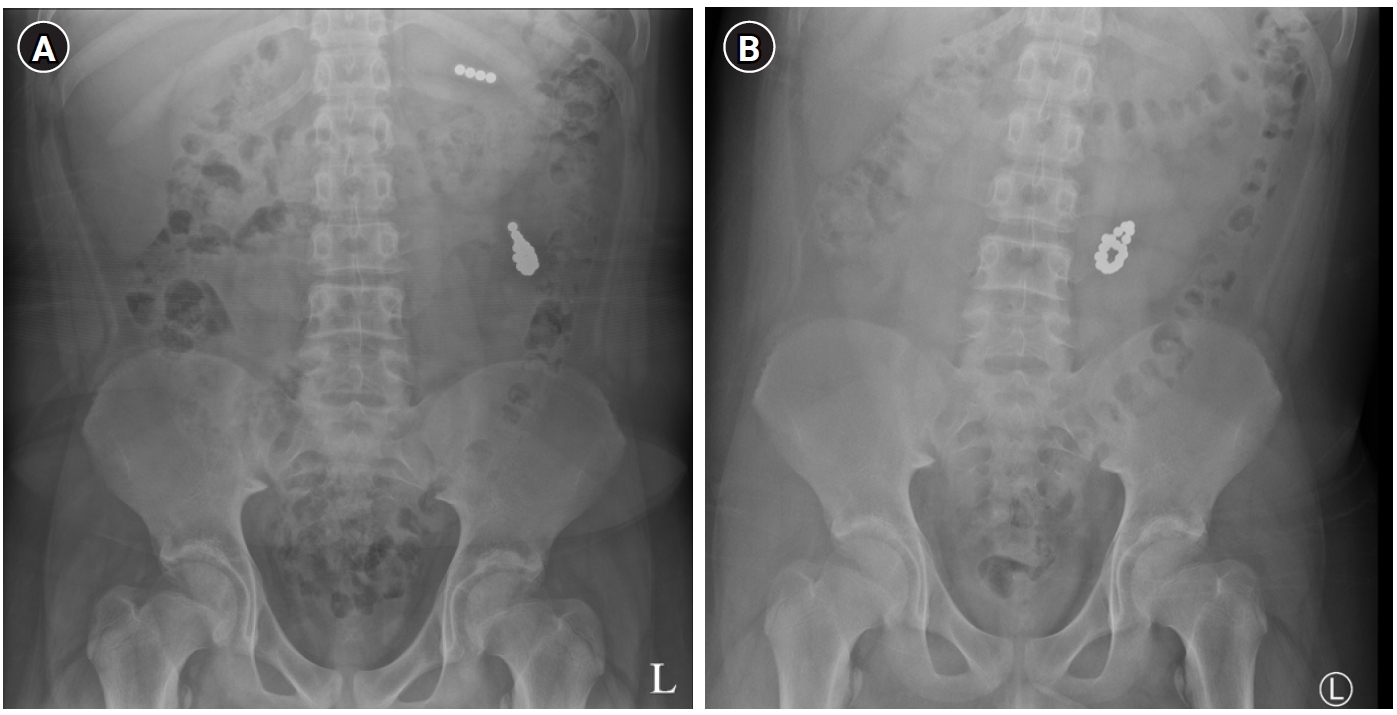
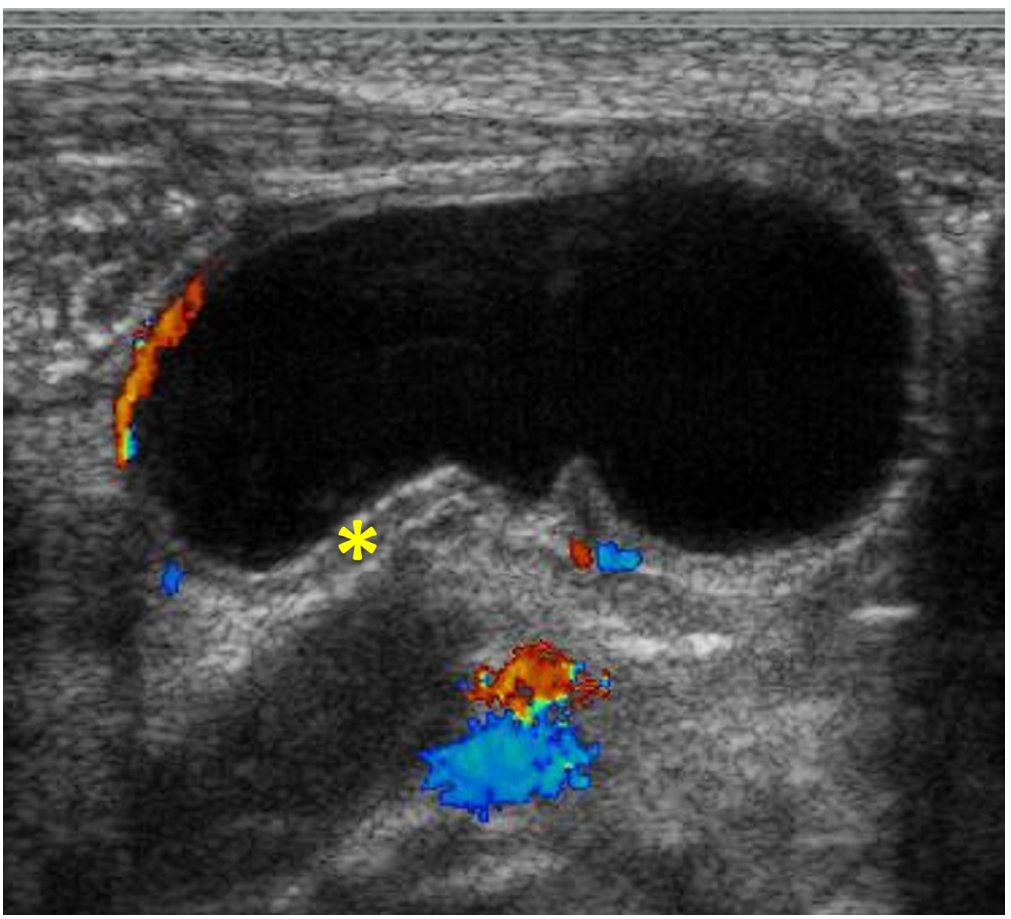
Debates exist about the appropriate treatment for pancreatic trauma in children. We intended to examine the safety of the operation of pancreatic trauma in children. This is a retrospective study of 13 patients, younger than 15, who underwent surgery for pancreatic trauma, between 1993 and 2011 in Seoul National University Children's Hospital. Medical records were reviewed for mechanism of trauma, clinical characteristics, radiological findings, operation and outcomes. Organ injury scaling from the AAST (American Association for Surgery of Trauma) was used. All injuries were caused by blunt trauma. Patients with grade III, IV, and those who were difficult to distinguish grade II from IV, underwent surgery due to severe peritonitis. Three patients with grade II were operated for reasons of mesenteric bleeding, tumor rupture of the pancreas, and progression of peritonitis. Distal pancreatectomy was performed in 10 patients and subtotal pancreatectomy and pylorus preserving pancreaticoduodenectomy in 1 patient each. The remaining one underwent surgical debridement because of severe adhesions. The location of injury, before and after operation, coincided in 83.3%. The degree of injury, before and after the operation, was identical in all the patients except for those who were difficult to tell apart grade II from grade IV, and those cannot be graded due to severe adhesion. Postoperative complications occurred in 23.1%, which improved with conservative treatment. Patients were discharged at mean postoperative 12(range 8~42) days. Even though patients with complications took longer in time from diagnosis to operation, time of trauma to operation and hospital stay, this difference was not significant. In conclusion, When pancreatic duct injury is present, or patient shows deterioration of clinical manifestation without evidence of definite duct injury, or trauma is accompanied by other organ injury or tumor rupture, operative management is advisable, and we believe it is a safe and feasible method of treatment.
Citations
Ketamine is a safe and effective drug for pediatric anesthesia, sedation and analgesia. We hoped to identify that surgeons could operate a pediatric hernia with the ketamine anesthesia without general anesthesia. The study was a consecutive case series of 2230 inguinal hernia patients aged 1 months to 17 years in a Joo's day-surgical clinic during 11-year period. The patients had pediatric inguinal hernia surgery without general anesthesia under the day-surgery system. We retrospectively analyzed the medical record of patients who were registered with the Diagnosis Related Group (DRG) system. All patients received ketamine (5mg/kg) and atropine (0.01mg/kg) intramuscularly before surgery. After anesthesia, we injected 1~2% lidocaine (Less than 5ml) subcutaneously at the site of incision and started operation. The surgical method was the high ligation method of the hernia sac.) In total 2230 patients, male were 1756 and female were 474. 2076 patients were a unilateral inguinal hernia at the time of surgery and 154 were bilateral hernia patients. Less than three months, depending on the age of the patients was 391, and less than 12 months the patient was 592 people (26.5%). After surgery, there were no accidents or long term complications associated with ketamine anesthesia. We think the surgeon can safely do the pediatric inguinal hernia surgery using ketamine and lidocaine without anesthesiologist through 11 years of our surgical experiences.
Fundoplication is a common surgical procedure for gastroesophageal reflux Disease (GERD). Recently the procedure has been performed with increased frequency laparoscopically. The aim of this study is to compare laparoscopic Nissen fundoplication (LNF) and open Nissen fundoplication (ONF) for GERD in children. We studied retrospectively the 88 pediatric patients who underwent the Nissen fundoplication for GERD as primary antireflux surgery from 1994 and 2009. ONF was performed in 34 cases and LNF was in 54 cases. 58 patients have neurologic impairment. Time to initial food intake after the surgery were reduced in the LNF group (
Experimental tracheal ligation (TL) has been shown to reverse the pulmonary hypoplasia associated with congenital diaphragmatic hernia (CDH) and to normalize gas exchange. The purpose of this study was to determine whether the TL would correct the surfactant deficiency present in the fetal rabbit model of CDH by using lamellar body count. Lamellar bodies are synthesized and secreted by the type II pneumocytes of fetal lung. The phospholipids present in these bodies constitute the major component of pulmonary surfactant. Twenty-one pregnant New Zealand rabbits underwent hysterotomy and fetal surgery on gestational day 24. Two fetuses of each pregnant rabbit were operated. In the fetus of one end of bicornuate uterus, left DH was created by excision of fetal diaphragm through open thoracotomy (DH Group). In the fetus of the other end of bicornuate uterus, left DH and TL were created (TL Group). The fetuses were delivered by Cesarean section on gestational day 31. Fourteen in control group, 12 in the DH group and 13 in TL group were born alive. En bloc excision of lungs, bronchi and trachea was done in all newborn rabbits. A five Fr catheter was inserted through trachea and repeated irrigations with 10 cc normal saline were done. The irrigated fluid was centrifuged at 280 xg for 5 minutes and the lamellar bodies were counted with the upper level fluid in platelet channel of electronic cell counter. The average lamellar body counts were 37.1 ± 14.2 × 103/µL in control group, 11.5 ± 4.4 × 103/#x00B5;L in DH group, and 6.5± 0.9 × 103/#x00B5;L in TL group. Lamellar body count in DH group was lower than in control group and did not increase after TL. This study shows TL has no therapeutic effect on decreased surfactant level of CDH and the pregnant rabbit is appropriate for the animal model of CDH.
Although laparoscopic surgery for hepatobiliary disease in children is possible, it is technically challenging. In an attempt to overcome these difficulties, the da Vinci Robotic Surgical System(R) was used to facilitate the minimally invasive treatment of choledochal cyst in six children. In early consecutive three cases, we experienced three complications; a case of laparotomy conversion, a case of late stenosis of the hepaticojejunostomy, and a case of leakage from a hepaticojejunostomy. However, in the last three cases the complete resection of the choledochal cyst and Roux-en-Y hepaticojejunostomy were performed using the robotic surgical system without complication.
We think robot-assisted choledochal cyst resection in children appears safe and feasible, and may increase the variety of complex procedures in pediatric surgical fields.
Citations
Biliary atresia (BA) is an infantile cholestatic disease of progressive obliterative cholangiopathy with varying degrees of damage to both extra and intrahepatic bile ducts due to unknown causes. The diagnostic studies should be done to diagnose or exclude BA without unnecessary delay. Kasai portoenterostomy is the first choice of treatment for bile drainage from microscopic bile ductules present in the portal fibrous mass. The medical management after Kasai portoenterostomy should be done carefully to maintain bile excretion and prevent and treat complications including cholangitis, hepatic fibrosis, portal hypertension and nutritional problem. The reported five years-survival rates after Kasai portoenterostomy range from 30 to 60%. About 20% of all patients undergoing Kasai portoenterostomy during infancy survive into adulthood with their native liver. Even if Kasai portoenterostomy remains as the first line of treatment in BA, liver transplantation serves as a good salvage treatment when portoenterostomy fails or liver function gradually deteriorates after initially successful establishment of bile flow. Overall 5-year survival rate in BA is about 90% in recent series.
Catheter related and perianal problems are common surgical complications encountered during the treatment of pediatric malignancies. However acute surgical abdominal emergencies are rare. The aim of this study is to review acute surgical abdominal complications that occur during the treatment of childhood malignancies. Out of a total of 1,222 patients who were newly diagnosed with malignant disease, between January 2003 and May 2008, there were 10 patients who required surgery because of acute abdominal emergencies. Their medical records were reviewed retrospectively. Hematologic malignancies were present in 7 patients (4 leukemia, 2 lymphoma, 1 Langerhans cell histiocytosis) and solid tumors in 3 patients (1 adrenocortical carcinoma, 1 desmoplastic small round cell tumor, 1 rhabdomyosarcoma). Seven patients had intestinal obstruction, two had gastrointestinal perforation and one, typhlitis. Intestinal obstructions were treated with resection of the involved segment with (N=2) or without (N=3) enterostomy. Two patients had enterostomy alone when resection could not be performed. Intestinal perforation was treated with primary repair. Typhlitis of the ascending colon was treated with ileostomy. Right hemicolectomy was necessary the next day because of the rapidly progressing sepsis. Three patients are now alive on chemotherapy and one patient was lost to followed-up. Among six patients who died, five died of their original disease progression and one of uncontrolled sepsis after intestinal perforation. Although rare, acute surgical abdominal complications can occur in childhood malignancies. Rapid and accurate diagnosis and appropriate operation are required for effective treatment of the complications.
A nationwide survey on acute appendicitis (AAP) was undertaken among members of the Korean Association of Pediatric Surgeons. The members were required to complete a questionnaire and the case registration form for each patient during the 6 months period from the 1st October, 2005 to 31st March, 2006. Questionnaires were collected from 23 members. Four hundred seventy six patients were registered from 21 hospitals where the members were working. The male to female ratio was 1.67:1. Average age was 9 years and 5 months (range 21 months-20 years). Operations were performed on average 10.4 hours (range 1-230 hours) from arrival at hospital. The average operation time was 59.1 minutes. The average admission days were 5.8 days (range 2-45 days). The most frequent symptoms were abdominal pain (95.1%), vomiting (50.6%) and fever (43.7%). The average duration of symptoms was 42.2 hours (range 1 hour-22 days). Leukocytosis (WBC count>10,000) was found in 85.9%. The most popular diagnostic tools were ultrasonography and CT. Open surgery was performed in 72.1% and laparoscopic surgery in 27.5%. Two laparoscopic surgeries were converted to open surgery (0.4%). Simple appendicitis was found in 54.5% and complicated appendicitis such as abscess, gangrenous change and perforation in 45.5%. According to the questionnaires 12 hospitals were performing open surgery only in all patients. Four hospitals were performing laparoscopic surgery in all patients. Seven hospitals are performing both surgical methods according to surgeon or occasion. Regarding the use of antibiotics in acute appendicitis, three kinds of antibiotics were used in 40% of total simple appendicitis patients. The results showed the trend of management in acute appendicitis in Korea. Especially it is necessary for the members to discuss the use of antibiotics for prophylaxis in the simple appendicitis
Citations
It is known that pediatric inguinal hernia is caused by the incomplete closure of processus vaginalis (PV). In the case of unilateral hernia, possibile contralateral patent PV should be considered because of its delayed appearance as well as its risk of incarceration. Direct visualization of patent PV could be done by contralateral exploration or by indirect exploration through the ipsilateral opening site of the affected hernia assisted with laparoscope. A patient group (321 persons) to whom laparoscopy was not performed from March 2000 to March 2003 was analyzed and compared with a patient group (280 persons) to whom laparoscopy was performed from April 2003 to September 2005. With all 601 patients, the sex ratio (male/female) of patients was 3.8:1. The side distribution was 57.7% in the right, 32.1% in the left and 10.1% in bilateral. There was no difference of sex and side distribution between before and after laparosopy adoption. We did not find an age correlation in natural closure of the residual PV of the peritoneum. Contralateral hernia developed in 14 persons (2.5%) after the operation of unilateral inguinal hernia before laparoscope adoption. But no contralateral hernia developed after April 2003 with laparoscopy. We think that if we use laparoscopy, being a safe and accurate method, to check whether the contralateral residual PV is opened or closed, possible future contralateral operation can be avoided.
We reviewed the records of 25 patients who were re-operated upon after primary repair of esophageal atresia with or without fistula at the Department of Pediatric Surgery, Seoul National University Children's Hospital, from January 1997 to March 2007. Types of the esophageal atresia anomalies were Gross type A in 5 patients, C in 18, and E in 2. The indications for re-operation were anastomosis stricture (n = 14), tracheo-bronchial remnant (n = 4), persistent anastomosis leakage (n = 3), recurrent tracheo-esophageal fistula (n = 2) and esophageal web (n = 2). The interval between primary and secondary surgery was from 48 days to 26 years 5 months (mean: 2 years and 4 months). Four patients required a third operation. The interval between the second and third operation was between 1 year 1 month and 3 year 10 month (mean: 2 years 5 months). Mean follow up period after last operation was 35 months (1 years–8 years 6 months). The secondary surgery was end-to-end esophageal anastomosis in 15, esophagoplasty in 5, gastric tube replacement in 5. After secondary operation, 6 patients had anastomosis stricture (4 patients were relieved of the symptoms by balloon dilatation, 2 patients underwent tertiary operation). Five patients had leakage (sealed on conservative management in all). Two patients had recurrent tracheo-esophagel fistula (1 patient received chemical cauterization and 1 patient underwent tertiary operation). Currently, only one patient has feeding problems. There were no mortalities. Secondary esophageal surgery after primary surgery for esophageal atresia was effective and safe, should be positively considered when complications do not respond to nonoperative therapy.
One day surgery in children has been practiced for last 10 years in this institution. This study is to examine its safety and effectiveness for patients younger than 15 years old treated at the Department of Pediatric Surgery, Asan Medical Center, from September. 1996 to December, 2005. A total of 3,709 patients, 37 % of the total pediatric operations, are included in this retrospective study. The most prevalent ages were between 1 and 3 years olds (1,199 patients). Twenty patients were younger than 6 months, and they all had one day surgery safely. Operations were herniorrhaphy in 3,126 patients,followed by excisional biopsy, chemoport removal, and OK 432 injection. There were 12 cases (0.32 %) of unplanned admissions, 7 occurred within 6 months of one day surgery. Perioperative fever was the most common cause of admission in 4 cases. The related conditions of unplanned admission were bleeding in 2 cases and radical surgery in 2. One day surgery in this institution was easily accessible and safe. This is to the result of appropriate selection of patients, cooperation with anesthesiologists, adequate control of postoperative pain, and home care programs.
Pediatric surgery could establish a definitive position in the medical field on the basis of a stable patient population. Neonatal surgery, the core of pediatric surgery, requires highly skilled surgeons. However, recent advancement of prenatal diagnosis followed by intervention and decreased birth rate has resulted in a significant decrease in the neonatal surgical population and the number of surgical operations. The purpose of this study is to examine the outcome of neonatal surgeries and to propose a guide for the future surgeries. A total of 359 neonatal surgical patients operated upon at the Department of Surgery, Ewha Medical Center, during past 21 years were studied. The study period hasbeen divided into two time periods : from 1983 to 1993 and from 1994 to 2004. Analysis was based on the Clinical Classification System and mortality pattern, frequency of disorders, occurrence and cause of death, and other changes. Neonatal surgery was 6.4 % of all pediatric surgery during the total 21 year period, 9.9 % in the first period and 4.8 % in the second. Male to female ratio increased from 2.7 : 1 to 2.1 : 1. The overall mortality was 6.7 %, and there was significant decrease from 7.4 % in the first period to 6.0 % in the second. The clinical classification system (CCS) for death cases included class II 2, III 4, and IV 7 during the first period and class III 3, and IV 8 during the second, respectively. According to the mortality pattern by Hazebroek, there were 6 preventable death cases during the first period, and only one in the second, and 2 non-preventable death cases during the first period and 8 in second, respectively. Although the patients in the second period had more serious diseases, surgical mortality has been decreased in the second period, which may be the result of improved surgery methods for newborns and advanced patient care.
Citations
Mature cystic teratoma, commonly called dermoid cyst, is the most common benign germ cell tumor of the ovary in children. Malignant transformation is rare, approximately 2%. As laparoscopic procedures are applied widely in pediatric surgery, a female chlid with a mature cystic teratoma may be an ideal candidate for laparoscopic surgery. Two children received laparoscopic operations successfuly for lower abdominal crises, twisted adnexa. There was no operative complication. Laparoscopic approach for ovarian lesions in infancy and childhood appears to be an effective and safe method for diagnosis as well as definitive therapy.
Hereditary pancreatitis (HP) appears as an autosomal dominant trait. If the patient has (1) more than 2 affected relatives in different generations and (2) no known etiological factors such as alcohol or gallstones, or has R122H or N29I mutation in the cationic trypsinogen (CT) gene, the diagnosis of HP can be applied. Risk of pancreatic cancer is estimated to be 53-fold higher than in a general population after the age of 50 years. We report a kindredof HP, involving three of its family together; two siblings (14 years old, 13 years old) and cousin (26 years old). The patient had complicating chronic pancreatitis and pancreatic stone, and was treated with amodified Puestow-Gillesby procedure. Her sisters showed chronic pancreatitis. Her cousin underwent a drainage procedure of the pancreatic duct for chronic pancreatitis during the high school period. All the three members showed the R122H mutation of the CT gene.
Citations
performed at the time of discharge. There was only one recurrence of adirect inguinal hernia. Necrotizing enterocolitis developed in 17 patients, 11 were operated upon, two had peritoneal drainages, and 9 had enterostomies. Five of 11 surgical infants died after operation and three of the nonsurgical infants died of various complications. Although micropremies have potentially high risks of serious complications and death, the outcome can improve with careful surgical observation and judgment.
Choledochal cysts have been associated with complications such as cholangitis, pancreatitis, and malignancy of the biliary tract. Recently, the incidence of choledochal cyst in neonate and young infant is increasing due to advances in diagnostic imaging. The aim of this study is to investigate the rationale of excision of choledochal cyst during the neonatal period. The clinical outcome and correlation between age at surgery and the degree of liver fibrosis were reviewed retrospectively. A total of 198 patients with choledochal cyst who were managed surgically between January 1985 and December 2000 at the Department of Surgery, Seoul National University Children's Hospital were included in this study. The overall outcome and the outcome of patients who were managed surgically during the neonatal period were compared. Correlation between age and the degree of liver fibrosis was evaluated by chi-square test and Pearson exact test. The mean age of the patients was 2 years 7 months (ranged from 5 days to 15 years). Mean postoperative follow-up period was 7 years 1 month (7 months to 20 years). The results are as follows. Twelve patients (6%) had postoperative complications, cholangitis (7), bleeding (4) and ileus (1). Eleven patients operated during the neonatal period had no postoperative complications. The positive correlation between age group and degree of liver fibrosis was statistically significant (chi-square: p=0.0165, Pearson exact test: p=0.019). The results support the rationale that excision of choledochal cyst can be performed safely without increasing morbidity in neonates.
A total of 30 cases of the peptic ulcer in children, who underwent operations from January 1981 to December 1995 because of complications at Department of the Surgery, Chonbuk National University Medical School, is reviewed. Twenty-three were males (76.7%), 7 females (23.3%) and male was preponderant at 3.3:1. There were 25 cases (83.3%) age 10 to 15 years, 3 (10.0%) between 2 and 9 years, and 2 (6.7%) below 2. The ulcer was located at duodenum in 27 (90.0%), and at stomach in 3 cases (10.0%). Complications were perforation in 19 cases (63.3%), pyloric obstruction in 9 (30.0%) and bleeding in 2 (6.7%). For perforation, truncal vagotomy with pyloroplasty was done in 11 cases, truncal vagotomy with hemigastrectomy and gastrojejunostomy in 6, and simple closure in 2 cases. For obstruction, truncal vagotomy with hemigastrectomy and gastrojejunostomy was done in 5, and truncal vagotomy and pyloroplasty in 3 cases. For bleeding lesions, truncal vagotomy and pyloroplasty was performed in 2 cases. Ten postoperative complications developed in 9 patients; adhesive ileus in 5, recurrence in 2, pneumonia 2, and wound seroma 1 case. One patient developed a primary duodenal perforation and another a recurrent obstruction. Both of patients had symptoms for more than 3 years and were treated with truncal vagotomy and pyloroplasty for the primary operations. Hospital stay was 11.5 days for the patient with perforated ulcer, 11.0 days for the patient with pyloric obstruction, and 14.5 days for the child with bleeding. Average hospital period was 11.6 days. To reduce recurrences after operation, extensive procedure such as distal gastrectomy with vagotomy at the first operation should be considered in case with severe complication or with patients who have been symptomatic for long periods.
Various surgical techniques for Hirschsprung's disease including total colonic aganglionosis have been performed with similar results. The type of redo pull-through procedure is determined by the cause of failure and the type of primary pull-through.
To understand the current status of neonatal surgery in Korea, a survey was made among the 36 members of the Korean Association of Pediatric Surgeons. The response rate was 75% (26 surgeons in 20 hospitals). Five hundred fifty three neonatal surgical patients treated in 1999 were analyzed. Regional numbers of patients were closely related to the regional population in most areas. Ano-rectal malformations (17%), pyloric stenosis (16%), Hirschsprung's disease (13%), atresia/stenosis of the gut (11%), esophageal atresia (8%) were the most common anomalies treated. The majority of operations were done within the first week of life. Seventy one per cent of cases were major life threatening or so-called neonatal index cases. Over-all mortality was 8 per cent. Higher mortality was observed in patients with diaphragmatic hernia (26%), gastro-intestinal perforation (18%), NEC (18%), and esophageal atresia(14%). Higher mortality was observed in patients with extremely low birth weight (33%) and low birth weight (18%). Associated anomalies were observed in 20%. Prenatal ultrasound was performed in 36 per cent with sensitivity of 20%. Result of this study was compared to the previous report (1994) and that of Japan (1998).
Congenital diaphragmatic hernia (CDH) in the past was considered a surgical emergency requiring immediate operation. Several groups now advocate preoperative stabilization and delayed surgery. The treatment strategy for CDH in this institution is delayed surgery after preoperative stabilization. The aim of this study was to evaluate the results of delayed surgery. A retrospective review of 16 neonates with CDH was performed. Surfactant, conventional mechanical ventilation, high frequency oscillation, and nitric oxide were utilized for preoperative stabilization as necessary. The difference in outcome between two groups differentiated by the duration of the preoperative stabilization periods with mechanical ventilation (≤ 8 hours and >8 hours) was determined. Chi-square test was used to analyze the data. There were 7 right-sided hernias and 9 left. The average duration of stabilization was 32.4 hours. Hepatic herniation through the defect was found in 6 cases and all died. The most common postoperative complication was pneumothorax. The mortality rate of the right side hernia was higher than the left (85.7% vs. 33.3%, p=0.036). Mortality rate of the group (N=8) whose preoperative stabilization period was 8 hours or less was better than that (N=6) whose preoperative stabilization period was more than 8 hours (25.0% vs. 83.3%, p=0.031). The overall mortality rate was 56.3%. The better prognosis was noticed in left side hernia, no liver herniation, or shorter preoperative stabilization period.
Henoch-Schonlein purpura is a systemic vasculitis of unknown etiology that is probably related to autoimmune phenomenon. Henoch-Schonlein purpura is characterized by purpuric rash, arthragia, nephritis, and gastrointestinal manifestations. We reviewed 169 children hospitalized with a diagnosis of Henoch-Schonlein purpura at Asan Medical Center between 1989 and 1998. One- hundred thirty-nine (82.2%) had gastrointestinal manifestations including abdominal pain, nausea, vomiting and gastrointestinal bleeding. Surgical consultations were obtained for ten children, and laparotomy was performed on five children. Three children suspected of appendicitis underwent appendectomy. None had the evidence of appendicitis. One child who was suspected of intestinal strangulation revealed, in pathologic review, the hemorrhagic edema of the proximal jejunum and of the distal ileum at laparotomy. Another child underwent resection for hemorrhagic infarct of distal ileum. High suspicion of this disease entity in differential diagnosis of abdominal pain in children can avoid unnecessary laparotomy in most cases. However, the life-threatening gastrointestinal complications may occur in a small percent of cases. The prompt recognition and adequate radiologic evaluation of abdominal manifestation of this entity is needed for an early surgical intervention.
Despite of advances in perinatal management and treatment modalities congenital diaphragmatic hernia(CDH) remains a frustrating problem. Although the sheep has proven to be a reliable experimental model for the production of intrauterine CDH, the rabbit may have some advantages. These include lower cost, smaller body size, year-round availability, high number of fetuses per pregnancy, and short gestational period. To evaluate the feasibility of the rabbit model of CDH, twenty-seven pregnant New Zealand rabbits were utilized. Hysterotomy and an operative procedure for creating a diaphragmatic defect on gestational day 24 or 25, in two fetuses of each pregnant rabbit were performed. In one fetus of one cornu of the uterus, the left fetal diaphragm was excised through an open thoracotomy(DH group). In another fetus in the other cornu, CDH was created and the trachea clipped(Surgiclip, USSC, Norwalk, Conn., USA) (TL group). Delivery was by Cesarean section on 30 days of gestation. Among twenty- seven pregnant rabbits, 12 in the DH group and eight in the TL group were born alive. The most common herniated organ was the left lobe of the liver. In thee DH group, the lungs were hypoplastic with decreased lung weightlbody weight ratio, reduced numbers of alveoli, thicker media of the pulmonary arteries, and immature alveoli. In TL group, the alveoli were more mature and did not differ from the control animals. In conclusion, (1) pulmonary hypoplasia develops in the fetal rabbit diaphragmatic hernia model and (2) simultaneous tracheal ligation prevents pulmonary hypoplasia.
This is a clinical review of 2,191 pediatric surgical patients under the age of 15 years, operated upon at the Division of Pediatric Surgery, Department of Surgery, Chonnam University Hospital from January 1988 to December 1997. The total number of operations in the pediatric age for all specialties were 13,144(13.2 %). The total operations including those performed on adults were 99,555. The most common age group operated upon was under 5 year of age(44.4 %). The number of operations in Division of General Pediatric Surgery were 2,191(16.7 %) out of total 13,144 operations in all pediatric specialties. The patients under 1 year of age in general pediatric surgery was 42.9 %(941/2,191). The most common diseases in neonates were anorectal malformation(20.6 %) and hypertrophic pyloric stenosis( 20.3 %). Infants older than neonates most commonly were operated upon for inguinal hernia(32.4 %) and intussusception(19.6 %). The total mortality rate in the neonatal intensive care unit was 31.3 %. Gastroschisis had the highest mortality.
Citations
To understand the current status of neonatal surgery in Korea, a suvey was made among the 27 members of Korean Association of Pediatric Surgeons. Response rate among surgeons was 78 perecnt, eighteen hospitals participated in this study. Five hundred and three cases of neonatal surgical patients were analyzed. In Korea, about 50% of cases were treated at the hospital in the capital city area. Regional number of patients were closely related to the regional population. Imperforate anus(19%), atresia/stenosis of gut(12%), and Hirschsprung's diseases(12%) were sitting at the top in the list. Majority of operation was done within the first week of life, especially during the first 24 hour period. Eighty per cent was major or so called index cases. Mortality in so-called index cases was 17%. High mortality was observed in patients with diaphragmatic hernia(47%), gastrointestinal perforation(65%) and esophageal atresia(28%). Low birth weight babies showed higher mortality in gastro -intestinal perforation, esophageal atresia and abdominal wall defect. These were compared to 1993 survey of Japanese Society of Pediatric Surgeons.
Citations
Citations
Citations
Citations
Citations
 First
First Prev
Prev

